Reduce payer friction, improve billing workflows, and support stronger reimbursement performance with behavioral-health-focused insurance knowledge built into the DENmaar platform.
Insurance Knowledge Team
Technology Alone
Doesn't Get Claims Paid.
Knowledge Does
Behavioral health reimbursement is constantly changing. Payer rules, modifiers, priorauthorizations, telehealth requirements, documentation standards, and state-specific billing policies create challenges that software alone cannot solve. DENmaar combines technology with a dedicated Insurance Knowledge Team focused exclusively on behavioral health reimbursement.
Behavioral Health Reimbursement Expertise
Operational support beyond software
Shared knowledge that strengthens outcomes

Built Specifically for Behavioral Health
Reimbursement support that understands
behavioral health complexity.
Our team works alongside providers and billing staff to navigate payer requirements, resolve
reimbursement issues, and continuously improve billing outcomes
Behavioral Health Expertise
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
Payer Intelligence
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
Continuous Research
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
Better Reimbursement
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
AREAS OF EXPERTISE
Commercial Insurance
Medicaid managed care
Medicare
Telehealth Billing
Prior Authorizations
Denial Management
Credentialing Support
Documentation Requirements
Behavioral Health Coding
How the Insurance Knowledge Team Works
A practical reimbursement support model that
turns payer complexity into operational clarity.
Every reimbursement issue becomes an opportunity to improve claim outcomes, strengthen workflows,
and make the DENmaar platform smarter over time.
1
Identify barriers
We identify reimbursement
challenges and payer roadblocks.
challenges and payer roadblocks.
2
Research Requirements
We research payer-specific requirements, rules, and policy updates.
3
Develop Strategy
We develop effective resolution strategies and best practices.
4
Share Knowledge
We share insights across the organization and client community.
5
Improve Workflows
We improve workflows to prevent recurring issues and denials.
6
Support Providers
We support providers
and billing teams every step of the way.
and billing teams every step of the way.
Knowledge That Improves the Entire Platform
Every reimbursement issue creates intelligence that strengthens future billing performance.
Every payer issue, denial pattern, workflow challenge, and reimbursement insight contributes to improving the DENmaar platform. The result is a continuously evolving system that becomes smarter over time—not just for one claim, but across operational billing workflows.
Payer issue patterns
Track the recurring payer requirements and billing obstacles that repeatedly affect reimbursement outcomes.
Denial insight loops
Use denial and follow-up experience to improve resolution quality and reduce repeat claim friction.
Workflow refinement
Translate reimbursement knowledge into better operational workflows tied to billing readiness and claim quality.
Shared organizational learning
Knowledge gained through real payer interactions can inform future reimbursement decisions across teams and clients.
Support for Multidisciplinary Organizations
Insurance knowledge support across the services and programs behavioral health organizations actually run.
DENmaar’s Insurance Knowledge Team supports organizations across outpatient therapy, psychiatry, substance use treatment, intensive programs, community behavioral health, and multidisciplinary care environments.
Therapy Practices
Medication Management
Substance Use Treatment Providers
IOP & PHP Programs
Community Behavioral Health Organizations
Multidisciplinary Practices
Why Organizations Choose DENmaar
Technology-supported workflows backed by real reimbursement knowledge.
DENmaar combines behavioral health specialization, reimbursement research, payer insight, and operational workflow support to help organizations improve billing accuracy and financial performance.
Behavioral health specialization
Real-world payer expertise
Continuous reimbursement research
Technology-supported workflows
Shared knowledge across client organizations
Focus on reimbursement accuracy
Request an Insurance Workflow Review
Discover how DENmaar’s Insurance Knowledge Team can strengthen reimbursement operations.
Request Information
TESTIMONIALS
WHAT OUR CLIENTS SAY
On behalf of everyone at Meadowlark Counseling Services, I want to extend our sincere thanks for the continued improvements you and your team have made to the DENMaar EMR platform. We have been consistently impressed with both the functionality and user-friendly design of the system, which has made a meaningful difference in our day-to-day operations. The intuitive layout and ease of use have allowed our staff to spend less time navigating the system and more time focusing on client care. The regular updates and enhancements reflect your commitment to meeting the evolving needs of providers in the behavioral health and substance use treatment fields. We genuinely look forward to the new features introduced each month and appreciate how responsive the platform has been to the demands of clinical workflows. We have been so pleased with our experience that we’ve taken the opportunity to recommend DENMaar to other professionals in Pennsylvania who are working in the SUD field. Thank you again for your ongoing support and partnership. We are grateful to be working with a company that truly understands the needs of its users. KIndly, Becky Parks on behalf of the entire team at Meadowlark Counseling Services
I referred one of my colleagues Dr Aaron to you he is just starting g his psychology private practice and looking at where to start. I told him hands down you guys are the best billers and have a great EMR and team. He said he reached out just wanted to let you know!
FANTASTIC job keeping things rolling along with any and all of our billing concerns as well as responding to other issues which may well have been out of your wheelhouse. We are VERY grateful to have you and the crew in our corner.
I appreciate you all so much and DENmaar has been such a blessing Donna to our overall operations and success as an expanding company—allowing us to ultimately operate more efficiently, get our claims paid more consistently, ad stay on top of the critical credentialing piece, among other things. Teamwork does in fact, make the dream work. I’ll loop Chris/Isabella in on this message thread too, as I want All of your team to be aware of how much we appreciate our working relationship with DENmaar
Thank you for your diligence!! I appreciate it so much. Thank you Edwina…
Thank you so much Amy! I will be referring to DENmaar as often as I am asked about credentialing services.
Our Latest Blogs
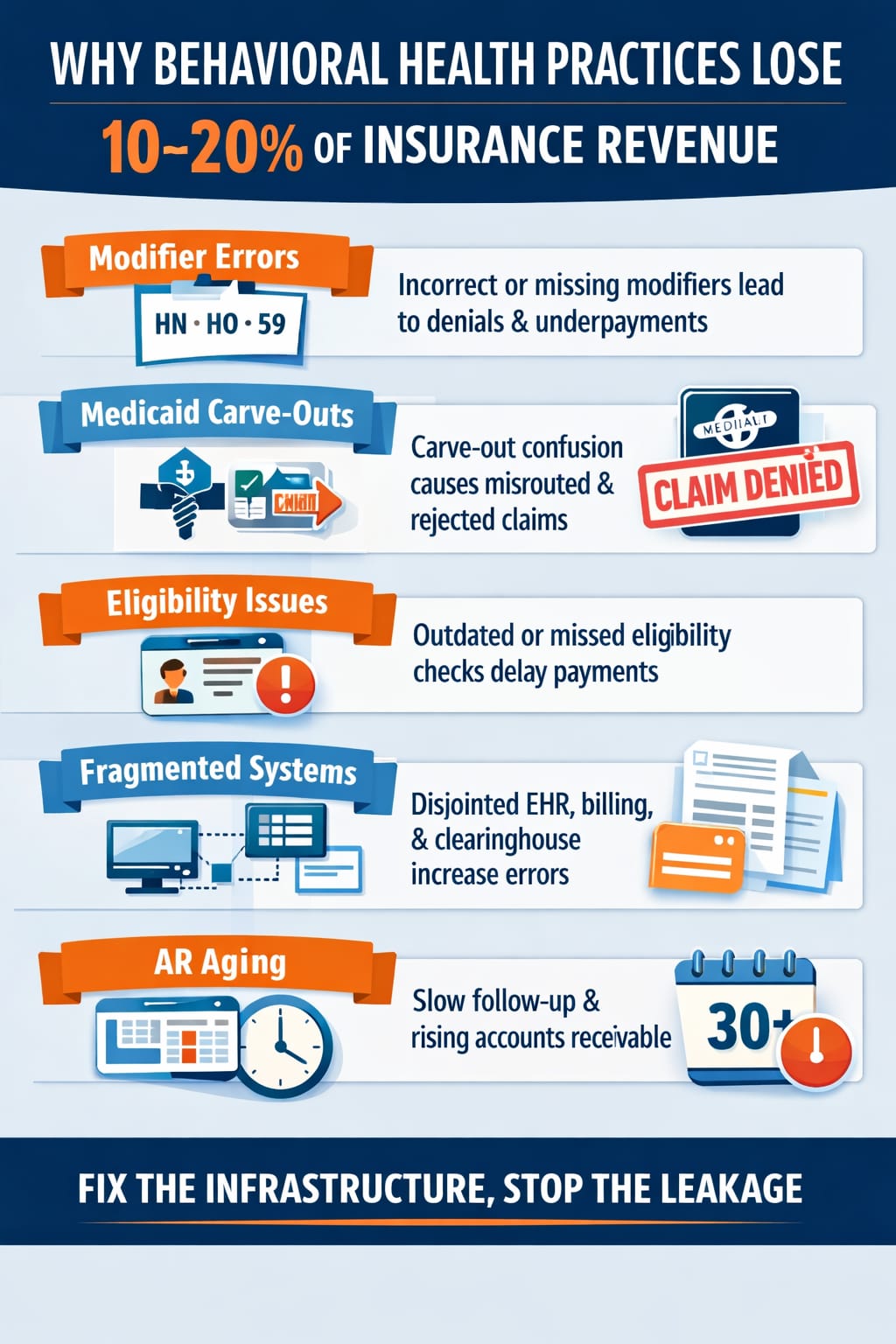
Why Behavioral Health Practices Lose 10 to 20 Percent of Insurance Revenue Without Realizing It
Most behavioral health practices believe their billing is “fine.”
Claims are going out. Payments are coming in. Denials do not look catastrophic.
But here is the uncomfortable reality:
Many practices quietly lose 10 to 20 percent of their insurance revenue, not because of fraud, incompetence, or bad providers, but because of structural claims friction.
Let’s break down where it actually leaks.
For a deeper system-level explanation, see claims hygiene in behavioral health billing.
1. Modifier Misalignment
Behavioral health is modifier heavy:
- HN / HO / HQ / HR
- 59 vs XE
- Facility vs professional billing logic
- State specific Medicaid rules
If modifier logic is not system enforced before submission, denials increase or worse, underpayments go unnoticed.
Small errors multiplied across thousands of Medicaid claims behavioral health submissions equal real revenue loss.
Without integrated behavioral health billing services and structured validation inside the EHR, modifier drift becomes systemic.
2. Medicaid Carve-Out Confusion
Behavioral health is often carved out from:
- Standard MCOs
- Commercial BCBS products
- State Medicaid networks
If eligibility verification does not detect carve-outs correctly, claims get routed incorrectly or denied after 30 or more days.
That is not a provider problem. That is infrastructure failure.
Strong behavioral health EHR and mental health EHR software systems must detect payer carve-outs before claims are generated.
3. Eligibility Gaps
Manual eligibility checks miss:
- Coverage changes
- Terminations
- Plan transitions
- Secondary payer coordination
A single eligibility miss can delay payment 45 to 60 days.
Multiply that across 15 to 20 providers and AR silently stretches.
Effective RCM for behavioral health requires real time eligibility logic built directly into the workflow, not spreadsheet tracking.
4. Fragmented Tools
Most practices operate with:
- Standalone EHR
- External biller
- Clearinghouse
- Manual tracking spreadsheets
- Email based follow up
Every handoff increases error probability.
Disconnected systems create invisible friction.
Integrated infrastructure, where EHR, documentation, and revenue cycle management operate together, reduces that friction significantly.
See how a technology plus services model works in practice
5. AR Aging Without Automation
If 30 day AR is not aggressively monitored and worked:
Revenue decays.
Most billing teams are reactive.
Top performing behavioral health revenue cycle management systems are proactive.
When claims infrastructure is engineered upstream, including structured documentation such as AI powered progress notes that align with payer rules, AR stabilizes and clean claims behavioral health performance improves.
The Difference Between Billing and Infrastructure
Billing is a task.
Infrastructure is a system that:
- Scrubs claims before submission
- Automates modifier logic
- Detects carve-outs
- Tracks AR aging in real time
- Reduces manual intervention
- Aligns compensation with collected revenue
When claims infrastructure is integrated directly into the EHR and RCM process, revenue leakage drops dramatically.
In our experience, many practices see 10 to 20 percent improvement in insurance revenue simply by eliminating friction.
Not by seeing more patients.
Not by raising rates.
By fixing structure.
Learn more about building infrastructure instead of chasing denials at DENmaar
Final Thought
If you do not measure:
- Clean claim rate
- Rejection percentage
- Denial percentage
- 0 to 30 day AR
- Cost per claim
You are not optimizing revenue.
You are hoping.
Hope is not a revenue strategy.
Frequently Asked Questions
Why do behavioral health practices lose insurance revenue?
Most revenue loss comes from modifier misalignment, Medicaid carve-out errors, eligibility gaps, and fragmented billing infrastructure rather than outright denials.
How much revenue leakage is normal in behavioral health billing?
Many practices unknowingly lose 10 to 20 percent of potential insurance revenue due to preventable structural issues in their EHR and revenue cycle workflow.
Does better billing staff fix revenue leakage?
Not alone. Revenue optimization requires system-level infrastructure that enforces payer rules, authorization logic, and clean claims standards before submission.
How can practices improve Medicaid behavioral health reimbursement?
By integrating eligibility detection, modifier enforcement, authorization tracking, and real time AR monitoring directly into their behavioral health EHR and RCM workflow.
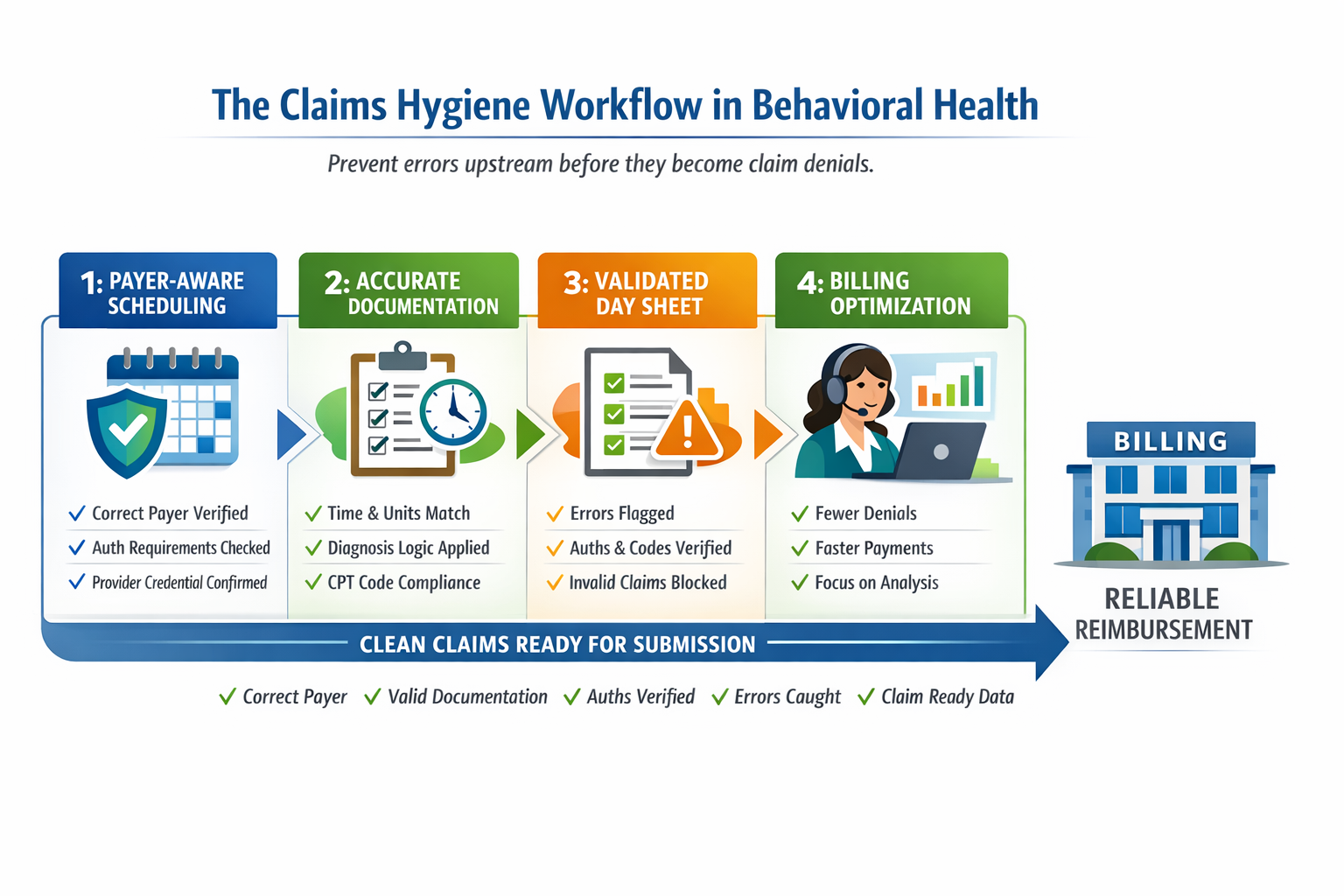
What “Claims Hygiene” Really Means in Behavioral Health
And Why Most Practices Are Fixing It Too Late
Most behavioral health practices think claim problems start in billing.
They don’t.
By the time a claim reaches a billing team, the outcome is already largely determined. Denials, rejections, underpayments are usually symptoms of upstream breakdowns that occurred days or weeks earlier inside the EHR.
We call this claims hygiene.
And if it is not engineered into your system, no amount of billing follow-up will fully fix it.
For a deeper breakdown of structured prevention, see claims hygiene in behavioral health billing.
Claims Hygiene Defined
Claims hygiene is the condition where every step before claim submission is structurally aligned to produce a payable claim by default.
That includes:
- Correct payer identification, especially mental health carve-outs
- Authorization-aware scheduling
- Time and unit accurate documentation
- Diagnosis logic that matches the service performed
- Day sheet logic that enforces payer rules before release
When these elements are clean and coordinated, billing becomes simple.
When they are not, billing becomes damage control.
This is not just a billing workflow. It is behavioral health revenue cycle management designed upstream inside the EHR.
Where Claims Actually Break (Upstream, Not in Billing)
In behavioral health billing, especially in Medicaid billing behavioral health environments, claim failure usually originates in one of four places:
1. Scheduling Without Payer Logic
Appointments are booked without confirming:
- The correct mental health payer
- Whether the service requires authorization
- Whether the provider is credentialed for that payer or program
Once the visit happens, the financial risk is already locked in.
Without integrated provider credentialing and insurance credentialing services awareness, scheduling becomes financially blind.
2. Documentation That Is Clinically Fine but Billing Unsafe
Notes often fail not because they are poor clinically, but because:
- Time thresholds do not match billed units
- Services rendered do not align with diagnosis logic
- Required elements for specific CPT or HCPCS codes are missing
Billing teams cannot fix documentation that was never structured correctly.
This is where structured AI documentation for behavioral health, including AI powered progress notes, becomes critical. Documentation must be payer aware, not just clinically complete.
3. Day Sheets That Do Not Enforce Rules
The day sheet is the last gate before claim submission and in many systems, it is passive.
If a day sheet allows:
- Invalid unit counts
- Missing authorizations
- Diagnosis and code mismatches
Then the system is allowing bad claims to exist.
A strong behavioral health EHR and mental health EHR software platform should enforce payer logic before claims are generated
4. Billing Teams Forced Into Manual Recovery
This is where most practices focus, but it is already too late.
At this stage, billing teams are:
- Correcting errors they did not create
- Appealing preventable denials
- Chasing missing information retroactively
This is not revenue cycle management. It is revenue triage.
True behavioral health billing services should prevent these breakdowns before submission.
Why “Clean Claims” Is the Wrong Goal
Many platforms advertise clean claim rates, but that metric is misleading.
A claim can be clean to a clearinghouse and still:
- Hit the wrong payer
- Violate MCO rules
- Fail authorization requirements
- Deny weeks later
True clean claims in behavioral health are payer true, service true, and rule true before submission ever happens.
This is especially critical in Medicaid claims behavioral health, psychiatry billing Medicaid, and substance use treatment billing environments where CMS 1500 versus UB 04 differences and managed care carve-outs matter.
Why Scaling Makes This Worse Fast
At 1 to 2 providers, errors are survivable.
At 10 or more providers:
- Small inconsistencies become systemic revenue loss
- Training breaks down
- Manual checks do not scale
- Billing headcount grows without fixing root causes
This is why many practices hit a ceiling where revenue plateaus despite growing volume.
Scaling requires system enforced behavioral health compliance, not manual memory.
What Real Claims Hygiene Looks Like
In a hygienic system:
- Insurance verification identifies mental health carve-outs automatically
- Scheduling is constrained by authorization and credentialing reality
- Documentation enforces time, units, and service logic
- Day sheets block invalid claims by design
- Billing teams focus on optimization, not cleanup
When this is in place, practices typically see:
- Fewer rejections and denials
- Faster payment cycles
- Lower billing staff burnout
- 10 to 20 percent improvement in realized insurance revenue without adding patients
This is the difference between submitting claims and building a revenue safe behavioral health system.
The Core Insight
Claims hygiene is not a billing function.
It is a system design problem.
If your EHR allows bad data to flow freely, billing will always be reactive.
If your system enforces payer aware logic upstream, billing becomes predictable and scalable.
Learn more about system level prevention at DENmaar.
Final Thought
Most practices do not need better billers.
They need fewer preventable mistakes.
Claims hygiene is not something you fix after the fact.
It is something you engineer into the workflow.
That is the difference between submitting claims and building a revenue safe system.
Frequently Asked Questions
What is claims hygiene in behavioral health billing?
Claims hygiene is the upstream enforcement of payer logic, authorization requirements, diagnosis alignment, and documentation accuracy before claims are submitted.
Why do Medicaid behavioral health claims deny so often?
Most denials stem from incorrect payer identification, missing authorizations, credentialing mismatches, or documentation errors created before billing ever sees the claim.
Can billing teams fix documentation errors?
No. Billing teams can correct coding or submission issues, but they cannot retroactively fix structurally flawed documentation.
How does an EHR improve clean claim rates?
A behavioral health EHR that enforces payer aware logic, authorization validation, and structured documentation reduces preventable denials before submission.
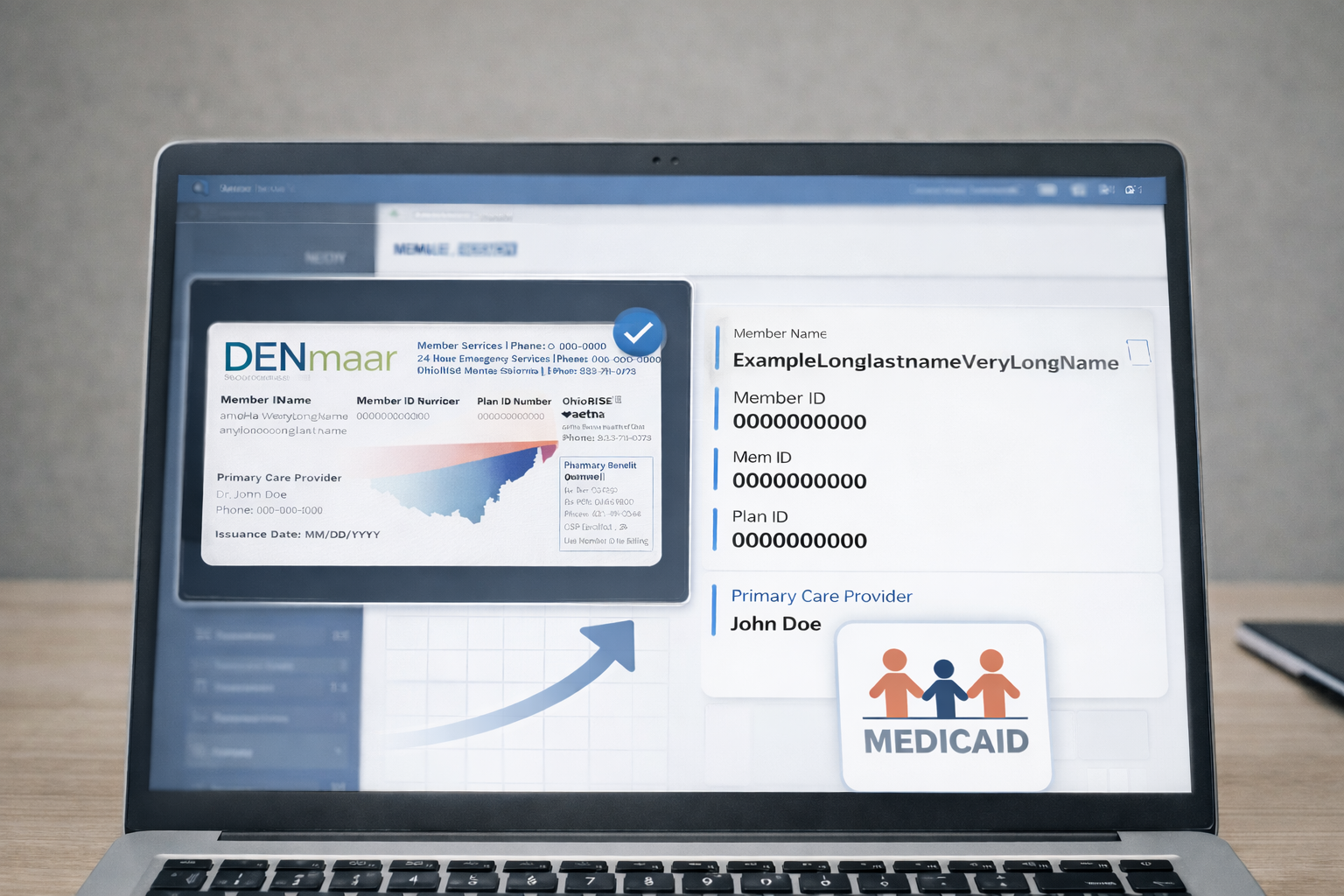
AI Insurance ID Card Reader for Mental Health Carve-Outs and Medicaid MCOs
Behavioral health billing has many pain points—documentation, coding, authorizations—but one of the most persistent is the insurance ID card itself.
Mental health benefits are often carved out from the medical plan. Medicaid members may be assigned to a medical MCO that is not the behavioral health payer. Insurance cards frequently list multiple phone numbers and logos with little clarity on who actually pays for services.
This is exactly the problem DENmaar’s AI Insurance ID Card Reader is designed to solve.
The Core Problem With Insurance ID Cards in Behavioral Health
In behavioral health, the payer printed on the insurance card is often not the payer you should bill.
Common scenarios include:
-
Commercial medical plans where mental health benefits are administered by Carelon Behavioral Health or Optum Behavioral Health
-
Medicaid members enrolled in a medical MCO while behavioral health is carved out to a separate entity
-
State-specific Medicaid structures where:
-
Physical health is billed to one payer
-
Mental health is billed to another
-
Substance use services may be billed to a third
-
Traditional EHR systems treat the insurance card as a static image. DENmaar treats it as structured intelligence.
How the AI Insurance ID Card Reader Works
When an insurance card is uploaded or captured, DENmaar’s AI does more than store it—it interprets it.
Automated Data Extraction
The AI reader extracts:
-
Payer name and plan name
-
Member ID and group number
-
Plan type (Medicaid, commercial, Medicare)
Behavioral Health Intelligence
The system:
-
Detects behavioral health carve-out indicators
-
Flags when the listed payer is medical-only
-
Triggers automated downstream verification logic
This transforms the insurance card into the first step of a clean claims workflow, not a future problem.
Mental Health Carve-Out Detection (The Key Differentiator)
DENmaar’s AI is trained specifically on behavioral health carve-out patterns, not generic eligibility rules.
Examples include:
-
Anthem or Blue Cross medical cards with mental health routed to Carelon
-
UnitedHealthcare medical plans with behavioral health managed by Optum
-
Medicaid MCO cards where behavioral health is administered by a state-designated carve-out entity
Instead of discovering these issues after denials, the system:
-
Flags carve-outs during intake
-
Assigns the correct behavioral health payer automatically
-
Prevents claims from being submitted to the wrong entity
This alone eliminates a large percentage of avoidable payer rejections.
Medicaid MCO Detection and Multi-Payer Awareness
Medicaid is where most EHRs struggle.
DENmaar’s AI Insurance ID Card Reader:
-
Recognizes state-specific Medicaid MCO card formats
-
Identifies when the MCO covers medical services only
-
Routes mental health services to the correct payer
-
Supports multi-payer logic across:
-
Therapy services
-
Psychiatry
-
Community-based care
-
Higher levels of care
-
This is critical for behavioral health organizations operating across multiple states with varying Medicaid rules.
Operational Impact for Behavioral Health Practices
For practices, this translates into:
-
Fewer intake errors
-
Cleaner eligibility records
-
Accurate payer mapping from day one
-
Fewer denials due to incorrect payer submission
-
Less staff time spent calling payers just to find the correct number
For DENmaar, it reinforces a core principle: save time while staying compliant.
Built for Scalable Behavioral Health Organizations
This system is not designed for one-off workflows or solo workarounds. It is built for:
-
Multi-provider practices
-
Multi-state behavioral health organizations
-
Medicaid-heavy patient populations
-
Teams that prioritize predictable cash flow over constant cleanup
For organizations planning to scale, this level of automation is no longer optional.
The Bigger Picture: Intake-to-Billing Intelligence
The AI Insurance ID Card Reader is not a standalone feature. It is a gateway to:
-
Accurate eligibility verification
-
Correct behavioral health payer assignment
-
Clean claims submission
-
Scalable, denial-resistant billing operations
It represents where DENmaar is headed: intake-to-billing intelligence built for how behavioral health actually works.
Our Partners
Ready to get started?
Feel free to reach out if you have any questions.