Reduce payer friction, improve billing workflows, and support stronger reimbursement performance with behavioral-health-focused insurance knowledge built into the DENmaar platform.
Insurance Knowledge Team
Technology Alone
Doesn't Get Claims Paid.
Knowledge Does
Behavioral health reimbursement is constantly changing. Payer rules, modifiers, priorauthorizations, telehealth requirements, documentation standards, and state-specific billing policies create challenges that software alone cannot solve. DENmaar combines technology with a dedicated Insurance Knowledge Team focused exclusively on behavioral health reimbursement.
Behavioral Health Reimbursement Expertise
Operational support beyond software
Shared knowledge that strengthens outcomes

Built Specifically for Behavioral Health
Reimbursement support that understands
behavioral health complexity.
Our team works alongside providers and billing staff to navigate payer requirements, resolve
reimbursement issues, and continuously improve billing outcomes
Behavioral Health Expertise
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
Payer Intelligence
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
Continuous Research
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
Better Reimbursement
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
AREAS OF EXPERTISE
Commercial Insurance
Medicaid managed care
Medicare
Telehealth Billing
Prior Authorizations
Denial Management
Credentialing Support
Documentation Requirements
Behavioral Health Coding
How the Insurance Knowledge Team Works
A practical reimbursement support model that
turns payer complexity into operational clarity.
Every reimbursement issue becomes an opportunity to improve claim outcomes, strengthen workflows,
and make the DENmaar platform smarter over time.
1
Identify barriers
We identify reimbursement
challenges and payer roadblocks.
challenges and payer roadblocks.
2
Research Requirements
We research payer-specific requirements, rules, and policy updates.
3
Develop Strategy
We develop effective resolution strategies and best practices.
4
Share Knowledge
We share insights across the organization and client community.
5
Improve Workflows
We improve workflows to prevent recurring issues and denials.
6
Support Providers
We support providers
and billing teams every step of the way.
and billing teams every step of the way.
Knowledge That Improves the Entire Platform
Every reimbursement issue creates intelligence that strengthens future billing performance.
Every payer issue, denial pattern, workflow challenge, and reimbursement insight contributes to improving the DENmaar platform. The result is a continuously evolving system that becomes smarter over time—not just for one claim, but across operational billing workflows.
Payer issue patterns
Track the recurring payer requirements and billing obstacles that repeatedly affect reimbursement outcomes.
Denial insight loops
Use denial and follow-up experience to improve resolution quality and reduce repeat claim friction.
Workflow refinement
Translate reimbursement knowledge into better operational workflows tied to billing readiness and claim quality.
Shared organizational learning
Knowledge gained through real payer interactions can inform future reimbursement decisions across teams and clients.
Support for Multidisciplinary Organizations
Insurance knowledge support across the services and programs behavioral health organizations actually run.
DENmaar’s Insurance Knowledge Team supports organizations across outpatient therapy, psychiatry, substance use treatment, intensive programs, community behavioral health, and multidisciplinary care environments.
Therapy Practices
Medication Management
Substance Use Treatment Providers
IOP & PHP Programs
Community Behavioral Health Organizations
Multidisciplinary Practices
Why Organizations Choose DENmaar
Technology-supported workflows backed by real reimbursement knowledge.
DENmaar combines behavioral health specialization, reimbursement research, payer insight, and operational workflow support to help organizations improve billing accuracy and financial performance.
Behavioral health specialization
Real-world payer expertise
Continuous reimbursement research
Technology-supported workflows
Shared knowledge across client organizations
Focus on reimbursement accuracy
Request an Insurance Workflow Review
Discover how DENmaar’s Insurance Knowledge Team can strengthen reimbursement operations.
Request Information
TESTIMONIALS
WHAT OUR CLIENTS SAY
On behalf of everyone at Meadowlark Counseling Services, I want to extend our sincere thanks for the continued improvements you and your team have made to the DENMaar EMR platform. We have been consistently impressed with both the functionality and user-friendly design of the system, which has made a meaningful difference in our day-to-day operations. The intuitive layout and ease of use have allowed our staff to spend less time navigating the system and more time focusing on client care. The regular updates and enhancements reflect your commitment to meeting the evolving needs of providers in the behavioral health and substance use treatment fields. We genuinely look forward to the new features introduced each month and appreciate how responsive the platform has been to the demands of clinical workflows. We have been so pleased with our experience that we’ve taken the opportunity to recommend DENMaar to other professionals in Pennsylvania who are working in the SUD field. Thank you again for your ongoing support and partnership. We are grateful to be working with a company that truly understands the needs of its users. KIndly, Becky Parks on behalf of the entire team at Meadowlark Counseling Services
I referred one of my colleagues Dr Aaron to you he is just starting g his psychology private practice and looking at where to start. I told him hands down you guys are the best billers and have a great EMR and team. He said he reached out just wanted to let you know!
FANTASTIC job keeping things rolling along with any and all of our billing concerns as well as responding to other issues which may well have been out of your wheelhouse. We are VERY grateful to have you and the crew in our corner.
I appreciate you all so much and DENmaar has been such a blessing Donna to our overall operations and success as an expanding company—allowing us to ultimately operate more efficiently, get our claims paid more consistently, ad stay on top of the critical credentialing piece, among other things. Teamwork does in fact, make the dream work. I’ll loop Chris/Isabella in on this message thread too, as I want All of your team to be aware of how much we appreciate our working relationship with DENmaar
Thank you for your diligence!! I appreciate it so much. Thank you Edwina…
Thank you so much Amy! I will be referring to DENmaar as often as I am asked about credentialing services.
Our Latest Blogs
Why Most Behavioral Health EHRs Fail at Billing And What a Billing-Optimized System Actually Looks Like
Behavioral health practices often assume billing problems come down to staff performance. Claims get rejected, payments are delayed, and revenue fluctuates unpredictably. The typical conclusion is that the billing team needs better training or more oversight.
In reality, the problem usually starts much earlier in the system architecture.
Most behavioral health EHRs were never designed to support efficient behavioral health revenue cycle management. Billing was added later as an auxiliary feature rather than built into the clinical workflow itself. This structural issue creates ongoing problems that practices attempt to solve with more staff, more manual review, and more time spent chasing claims.
The result is predictable: lost revenue, administrative friction, and frustrated providers.
Modern organizations increasingly rely on integrated platforms like behavioral health EHR and mental health practice management software designed to align clinical workflows with billing accuracy and Medicaid reimbursement requirements.
The Structural Problem With Most EHRs
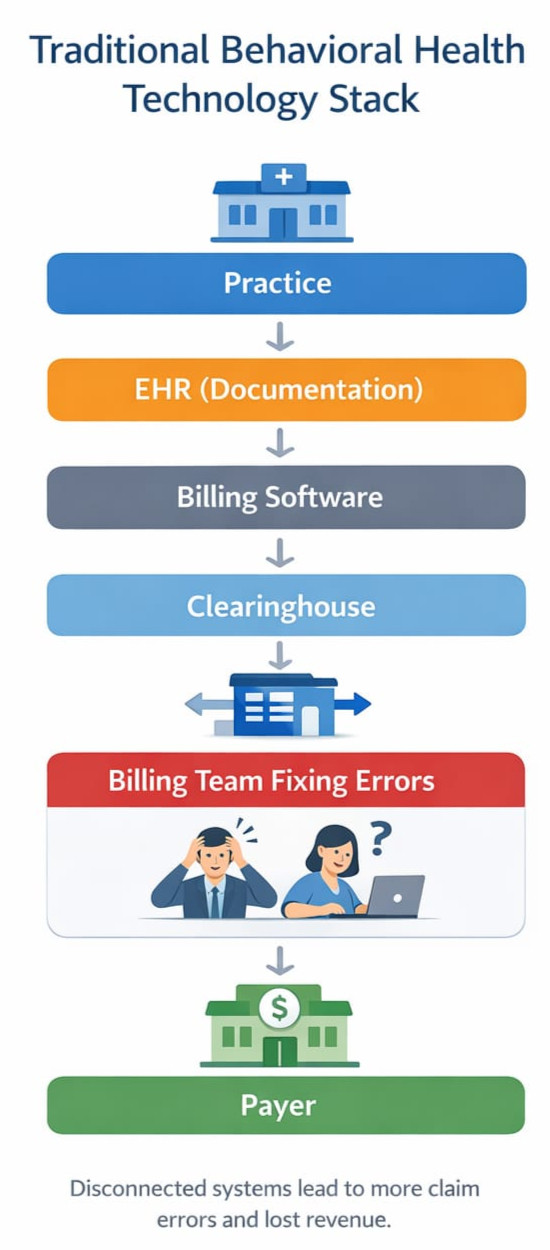
The traditional behavioral health technology stack looks something like this:
Practice → EHR → Billing Software → Clearinghouse → Billing Team
Each layer operates somewhat independently. Documentation is completed inside the EHR, then billing staff extract the information needed to generate claims. If documentation is incomplete, inconsistent, or coded incorrectly, the claim fails downstream.
This architecture introduces several common problems.
Documentation and Billing Are Disconnected
Clinical notes are written for clinical purposes, not claim validation. Important billing elements such as time requirements, service modifiers, or diagnosis linkage may not be captured correctly in the workflow.
Modern systems increasingly solve this problem through structured documentation and AI progress notes for behavioral health, ensuring that clinical documentation supports both care delivery and billing compliance.
Errors Are Discovered Too Late
In many systems, claim validation occurs only after the claim is generated and submitted. By that point, rejections or denials require additional staff intervention.
Eligibility and Payer Rules Are Separate From Clinical Workflow
Eligibility verification and payer specific requirements often live outside the EHR entirely. Front desk staff, clinicians, and billing teams operate with incomplete information about payer policies.
Claims Follow Up Becomes Labor Intensive
When problems occur, billing teams spend hours tracking down documentation errors, contacting payers, or correcting claims.
None of these problems are fundamentally about the billing staff.
They are system design problems.
The Real Cost of Fragmented Billing Systems
Behavioral health practices frequently underestimate how much revenue is lost through inefficient billing infrastructure.
Common revenue leakage points include:
- Incorrect or missing modifiers
- Mismatched documentation and CPT codes
- Eligibility verification failures
- Incorrect claim forms such as CMS-1500 vs UB-04
- Incomplete prior authorization tracking
- Delayed follow up on rejected claims
Across the industry, these issues typically reduce collected revenue by 10–20%.
Many organizations are unaware that behavioral health providers lose 10–20 percent of insurance revenue due to inefficiencies in billing workflows and claims management.
For many practices, that difference determines whether they are able to hire additional clinicians, expand services, or invest in better care infrastructure.
What a Billing-Optimized Behavioral Health EHR Looks Like
If billing performance depends on system architecture, the logical solution is to design the clinical system around revenue cycle integrity from the beginning.
A billing optimized behavioral health platform integrates several core elements directly into the workflow.
Documentation That Drives Coding
Clinical documentation should guide coding decisions rather than leaving coding entirely to billing staff. Structured note elements help ensure that required billing information such as time thresholds, service type, and diagnosis linkage is captured during the clinical encounter.
Integrated Eligibility and Payer Intelligence
Eligibility verification and payer rules should be visible within the system before services occur. This allows practices to confirm coverage, identify authorization requirements, and avoid preventable claim failures.
Pre Submission Claim Validation
Claims should be evaluated and scrubbed before submission to clearinghouses. Identifying errors upstream prevents the cycle of rejection, correction, and resubmission that slows revenue flow.
Maintaining strong claims hygiene in behavioral health billing is one of the most effective ways to improve clean claims rates and Medicaid reimbursement.
Continuous Claims Monitoring
Billing does not end at submission. Effective systems monitor claim status, identify payer responses, and intervene when issues arise.
Support for Multiple Billing Models
Behavioral health organizations increasingly operate across multiple service levels and billing structures. Systems must support both CMS-1500 professional claims and UB-04 institutional claims depending on the services provided.
Without this flexibility, practices are forced to maintain multiple disconnected systems.
Many organizations address this complexity through specialized behavioral health billing services and integrated revenue cycle management solutions.
Why This Matters for Behavioral Health
Behavioral health reimbursement is particularly complex compared with many other healthcare sectors.
Practices frequently operate across multiple disciplines including:
- Therapy
- Psychiatry
- Substance use disorder treatment
- Intensive outpatient programs (IOP)
- Community based services
- Case management
Each service category introduces different coding requirements, payer rules, and claim forms.
If billing logic is not integrated directly into the clinical infrastructure, the administrative burden grows rapidly as practices expand.
This is one reason many behavioral health organizations struggle to scale.
The Future of Behavioral Health Infrastructure
Over time, behavioral health technology will move away from isolated software tools toward integrated operating systems for practices.
In this model, documentation, billing, credentialing, communication, and analytics are connected within a unified platform.
Clinical workflow generates structured data that feeds directly into revenue cycle processes. Claims validation occurs automatically before submission. Eligibility, authorizations, and payer rules are continuously integrated into the system.
Platforms like DENmaar EHR are built around this concept, combining behavioral health documentation, billing workflows, and revenue cycle management into a single system.
The result is a much more stable and predictable revenue cycle.
The Results of an Integrated Approach
When billing architecture is built directly into the platform, claim performance improves dramatically.
At DENmaar, for example, practices operating within an integrated clinical and revenue cycle system currently achieve:
- 98.1% clean claims
- 1.47% rejected claims
- 0.32% denied claims
Those numbers place performance within the top tier of healthcare revenue cycle outcomes.
More importantly, practices using integrated systems typically experience 10–20% increases in insurance revenue simply by reducing claim friction and administrative leakage.
The Takeaway
When billing problems arise, it is easy to assume the issue lies with the billing team.
In many cases, the real cause is the technology architecture supporting the revenue cycle.
Behavioral health practices that want to grow sustainably need systems designed around billing integrity from the start rather than systems where billing is an afterthought.
As behavioral health services continue to expand and payer requirements grow more complex, billing optimized infrastructure will increasingly define which organizations succeed.
And which ones continue struggling with the same avoidable claim problems.
Frequently Asked Questions
Why do most behavioral health EHR systems struggle with billing?
Many behavioral health EHR platforms were originally designed for clinical documentation rather than revenue cycle management. Because billing was added later, documentation workflows, payer rules, and claim validation are often disconnected.
What is behavioral health revenue cycle management?
Behavioral health revenue cycle management refers to the full process of managing insurance claims, eligibility verification, coding, billing, and reimbursement for mental health and substance use treatment services.
Why are clean claims important in behavioral health billing?
Clean claims are insurance claims submitted without errors or missing data. Strong claims hygiene improves approval rates, reduces denials, and accelerates Medicaid behavioral health reimbursement.
How can AI improve behavioral health documentation and billing?
AI tools can automate clinical documentation and generate structured progress notes that align with billing requirements. This helps clinicians reduce administrative work while improving billing accuracy.

Why Behavioral Health Needs a New Operating Model
Multidisciplinary Care, Dual Claim Systems, and the Rise of Claims Hygiene
Behavioral health is changing.
Over the past decade, the industry has expanded beyond traditional outpatient therapy into a much broader continuum of care. Today’s practices increasingly include multiple service lines:
- Outpatient therapy
- Psychiatry and medication management
- Substance use disorder (SUD) treatment
- Intensive outpatient programs (IOP)
- Partial hospitalization programs (PHP)
- Community-based services
- Residential programs such as ASAM 3.1
Yet the technology supporting many of these organizations still assumes a simple model: one provider, one discipline, one claim type.
That assumption no longer holds.
Modern behavioral health organizations require systems designed around multiple disciplines, multiple billing frameworks, and increasingly complex payer rules.
The practices that understand this shift are building something fundamentally different.
For many organizations, adopting a modern behavioral health EHR platform and integrated behavioral health revenue cycle management approach is the first step toward solving these challenges.
The Multidisciplinary Behavioral Health Organization
The most resilient behavioral health organizations today are not single-service clinics.
They are multidisciplinary systems of care.
A single organization might include:
- Licensed therapists
- Psychiatrists and psychiatric nurse practitioners
- SUD counselors
- Case managers
- Community support specialists
- Residential program staff
Each discipline introduces different documentation standards, payer expectations, and billing structures.
A therapy session may be billed as CPT 90837, while case management could use T1016, and an intensive outpatient day might involve a facility-based service with entirely different billing rules.
Trying to run this ecosystem on software designed only for therapy quickly creates friction.
This is where the distinction between professional claims and facility claims becomes critical.
Many organizations discover they are losing significant insurance revenue due to billing inefficiencies, something explored in detail in this analysis of how providers lose 10–20% of insurance revenue due to revenue cycle gaps.
CMS-1500 vs UB-04: Two Claim Worlds in Behavioral Health
Behavioral health providers often operate across two fundamentally different claim systems.
Understanding CMS 1500 vs UB 04 billing is essential for accurate Medicaid behavioral health reimbursement and clean claims.
CMS-1500 (Professional Claims)
Used for services delivered by individual clinicians such as:
- Therapy sessions
- Psychiatric evaluations
- Medication management
- Individual counseling
These claims are built around:
- CPT / HCPCS procedure codes
- Rendering provider information
- Service units and modifiers
This is the traditional model most EHRs support.
But it is only half the story.
UB-04 (Facility Claims)
Programs such as IOP, PHP, residential treatment, and some SUD services may require facility billing.
These claims rely on a completely different structure:
- Revenue codes
- Facility identifiers
- Program-level billing logic
- Episode-based service tracking
Many organizations running these services discover that their EHR cannot properly support UB-04 workflows.
As a result, staff often build manual workarounds, spreadsheets, and external billing processes.
The operational cost of this fragmentation is enormous.
This is why many providers adopt specialized behavioral health billing services designed for complex Medicaid and multi-program organizations.
The Hidden Problem: Claims Hygiene in Behavioral Health Billing
Even with the right claim format, most behavioral health revenue cycles struggle with something far more basic.
Data integrity.
We call this claims hygiene in behavioral health billing.
Claims hygiene refers to the accuracy and completeness of the information required to produce a clean claim:
- Correct insurance identification
- Accurate payer routing
- Valid provider credentials
- Proper service coding
- Diagnosis linkage
- Authorization verification
- Clean eligibility data
When these elements are wrong or incomplete, claims fail.
The result is familiar to many organizations:
- Rising denial rates
- Aging receivables
- Administrative overload
- Lost revenue
Improving claims hygiene is often the fastest way to increase revenue without seeing a single additional patient.
Where Most Behavioral Health Systems Fail
Many EHR platforms were originally designed for small outpatient therapy practices.
They assume a simple model:
One clinician
One note
One claim
But multidisciplinary behavioral health organizations operate in a very different reality.
They need systems capable of supporting:
- Multiple clinical disciplines
- CMS-1500 professional claims
- UB-04 facility claims
- Complex Medicaid program structures
- Integrated behavioral health revenue cycle management workflows
Without this architecture, billing becomes an afterthought rather than an integrated system.
Organizations increasingly turn to purpose-built platforms like DENmaar EHR, designed specifically for behavioral health compliance, Medicaid billing workflows, and multi-program organizations.
The Future: Integrated Behavioral Health Operating Systems
The next generation of behavioral health platforms will not separate clinical documentation from revenue cycle management.
Instead, they will treat documentation, scheduling, and billing as a single operational system.
This means:
- Services mapped to claim type (CMS-1500 or UB-04)
- Documentation structured to support billing requirements
- Eligibility and payer data captured early in the workflow
- Claims validated before submission
When this approach is implemented correctly, organizations see dramatic improvements:
- Higher clean claim rates
- Faster reimbursements
- Reduced administrative workload
- More predictable revenue
Modern platforms are also introducing AI progress notes for behavioral health, allowing clinicians to automate documentation while maintaining compliance with billing requirements.
A System Designed for the Real Behavioral Health Market
The behavioral health industry is not simple.
It spans therapy, psychiatry, substance use treatment, residential care, and community-based services.
Technology must reflect that complexity.
The organizations that thrive in the next decade will be those that build systems around three principles:
- Multidisciplinary care delivery
- Support for both CMS-1500 and UB-04 claim structures
- Operational discipline around claims hygiene
This is not just a billing strategy.
It is a new operating model for behavioral health.
Frequently Asked Questions
What is the difference between CMS-1500 and UB-04 in behavioral health billing?
CMS-1500 is used for professional claims submitted by individual providers such as therapists and psychiatrists. UB-04 is used for facility-based services like intensive outpatient programs, residential treatment, and hospital services.
Why is claims hygiene important in behavioral health revenue cycle management?
Claims hygiene ensures that all billing data such as insurance information, provider credentials, and service codes are accurate before submission. Strong claims hygiene improves clean claims rates, Medicaid reimbursement, and behavioral health revenue cycle performance.
What software do behavioral health organizations need?
Modern organizations require behavioral health EHR systems with integrated billing, Medicaid claims support, and AI documentation tools to manage multidisciplinary care and complex billing workflows.
How can AI help behavioral health documentation?
AI documentation tools can generate AI progress notes and clinical summaries, reducing clinician workload while ensuring notes meet compliance and billing requirements.
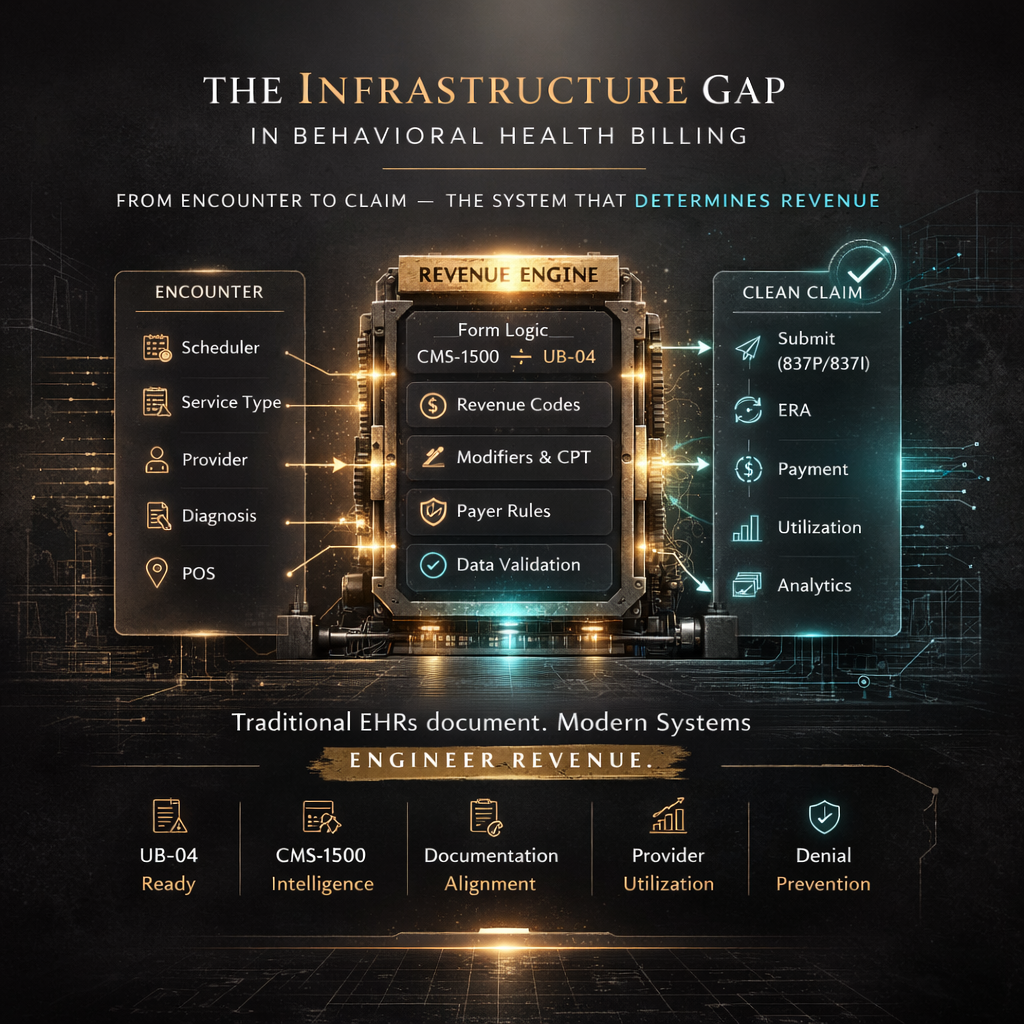
The Infrastructure Gap in Behavioral Health Billing
Why most EHR platforms were never designed for complex revenue
Behavioral health has a revenue problem and it isn’t payer rates.
It’s infrastructure.
Most EHR platforms were designed for documentation first, billing second. That model works for solo therapy practices submitting basic CMS-1500 claims. It breaks down the moment complexity enters the picture.
And complexity is now the rule, not the exception.
For many organizations, this structural gap is one of the reasons behavioral health practices lose 10–20% of insurance revenue without realizing it.
Where Systems Begin to Fail
As practices expand into:
- Intensive Outpatient Programs (IOP)
- Community Mental Health (CMHC) services
- ACT, PSR, and H2038 programs
- Multi-discipline care models
- Medicaid Managed Care carve-outs
They encounter a structural reality:
CMS-1500 logic alone is not enough.
UB-04 becomes necessary. Revenue codes become necessary. Type-of-Bill fields matter. Rendering vs. attending provider logic matters. Diagnosis pointers and modifiers are no longer optional details — they are claim survival requirements.
Yet most platforms treat these as add-ons, not core architecture.
That’s the gap.
Without strong behavioral health billing services and revenue cycle management infrastructure, these requirements create systemic claim friction.
The Encounter to Claim Disconnect
In many systems:
Scheduler → Note → Claim
are loosely connected.
But in complex billing environments, these must be unified.
At the encounter level, the system must already know:
- Whether the service maps to CMS-1500 or UB-04
- What revenue code is required
- What modifiers are payer-specific
- Which provider field populates where
- How diagnosis pointers align to CPT lines
- What place of service logic applies
If this logic is not embedded upstream, denial management becomes downstream chaos.
Strong behavioral health EHR and mental health EHR software must align documentation, billing rules, and payer requirements before a claim is generated.
Clean Claims Are an Architectural Outcome
High clean-claim rates are not achieved by working harder.
They are achieved by designing systems where:
- Documentation aligns with billing requirements
- Service types control form type automatically
- Revenue codes are required when necessary
- Payer rule tables are embedded
- Eligibility carve-outs are detected before submission
This approach reflects the concept of claims hygiene in behavioral health billing, where payer rules and documentation logic are enforced upstream.
When infrastructure is correct, denials decline structurally.
When infrastructure is weak, billing teams become firefighters.
Utilization Is Revenue, Not Just Scheduling
A second infrastructure blind spot is provider utilization.
Behavioral health revenue is directly tied to:
- Delivered units
- Authorization alignment
- Cancellation management
- Provider productivity
If your system cannot measure utilization accurately, it cannot optimize revenue.
In percentage-based revenue models, this alignment becomes even more critical.
Structured clinical documentation, including AI-assisted progress notes for behavioral health, can also support payer-aligned billing accuracy and improve clean claims performance.
The Shift That’s Coming
The era of disconnected tools is fading.
Documentation, billing logic, and utilization reporting must converge into a single revenue-intelligent engine.
Behavioral health is becoming more complex, not less. Medicaid programs are expanding. Multi-discipline care models are growing. Compliance scrutiny is increasing.
Infrastructure must mature accordingly.
The practices that win over the next decade will not simply document well.
They will design their revenue systems deliberately.
Organizations building scalable behavioral health infrastructure increasingly rely on integrated systems such as DENmaar’s behavioral health platform.
No hype.
No promises.
Just structural clarity.
Frequently Asked Questions
Why do many behavioral health EHR systems struggle with complex billing?
Many EHR platforms were originally designed for documentation rather than revenue cycle management. When organizations add services like IOP, CMHC programs, or Medicaid-based care, the billing complexity exceeds the system’s original architecture.
What is the difference between CMS-1500 and UB-04 billing in behavioral health?
CMS-1500 forms are typically used for professional services such as therapy and psychiatry. UB-04 forms are used for institutional services such as IOP or facility-based care where revenue codes and type-of-bill fields are required.
What is behavioral health claims hygiene?
Claims hygiene refers to structuring documentation, payer logic, eligibility verification, and billing rules so that claims are correct before submission, reducing denials and improving clean claim rates.
Why is revenue cycle infrastructure important for Medicaid behavioral health billing?
Medicaid behavioral health programs often include carve-outs, unique modifiers, HCPCS codes, and authorization rules. Without integrated infrastructure inside the EHR and billing workflow, practices experience denials, delays, and revenue leakage.
Our Partners
Ready to get started?
Feel free to reach out if you have any questions.