Reduce payer friction, improve billing workflows, and support stronger reimbursement performance with behavioral-health-focused insurance knowledge built into the DENmaar platform.
Insurance Knowledge Team
Technology Alone
Doesn't Get Claims Paid.
Knowledge Does
Behavioral health reimbursement is constantly changing. Payer rules, modifiers, priorauthorizations, telehealth requirements, documentation standards, and state-specific billing policies create challenges that software alone cannot solve. DENmaar combines technology with a dedicated Insurance Knowledge Team focused exclusively on behavioral health reimbursement.
Behavioral Health Reimbursement Expertise
Operational support beyond software
Shared knowledge that strengthens outcomes

Built Specifically for Behavioral Health
Reimbursement support that understands
behavioral health complexity.
Our team works alongside providers and billing staff to navigate payer requirements, resolve
reimbursement issues, and continuously improve billing outcomes
Behavioral Health Expertise
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
Payer Intelligence
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
Continuous Research
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
Better Reimbursement
Our team specializes exclusively
in behavioral health reimbursement
across all payer types.
in behavioral health reimbursement
across all payer types.
AREAS OF EXPERTISE
Commercial Insurance
Medicaid managed care
Medicare
Telehealth Billing
Prior Authorizations
Denial Management
Credentialing Support
Documentation Requirements
Behavioral Health Coding
How the Insurance Knowledge Team Works
A practical reimbursement support model that
turns payer complexity into operational clarity.
Every reimbursement issue becomes an opportunity to improve claim outcomes, strengthen workflows,
and make the DENmaar platform smarter over time.
1
Identify barriers
We identify reimbursement
challenges and payer roadblocks.
challenges and payer roadblocks.
2
Research Requirements
We research payer-specific requirements, rules, and policy updates.
3
Develop Strategy
We develop effective resolution strategies and best practices.
4
Share Knowledge
We share insights across the organization and client community.
5
Improve Workflows
We improve workflows to prevent recurring issues and denials.
6
Support Providers
We support providers
and billing teams every step of the way.
and billing teams every step of the way.
Knowledge That Improves the Entire Platform
Every reimbursement issue creates intelligence that strengthens future billing performance.
Every payer issue, denial pattern, workflow challenge, and reimbursement insight contributes to improving the DENmaar platform. The result is a continuously evolving system that becomes smarter over time—not just for one claim, but across operational billing workflows.
Payer issue patterns
Track the recurring payer requirements and billing obstacles that repeatedly affect reimbursement outcomes.
Denial insight loops
Use denial and follow-up experience to improve resolution quality and reduce repeat claim friction.
Workflow refinement
Translate reimbursement knowledge into better operational workflows tied to billing readiness and claim quality.
Shared organizational learning
Knowledge gained through real payer interactions can inform future reimbursement decisions across teams and clients.
Support for Multidisciplinary Organizations
Insurance knowledge support across the services and programs behavioral health organizations actually run.
DENmaar’s Insurance Knowledge Team supports organizations across outpatient therapy, psychiatry, substance use treatment, intensive programs, community behavioral health, and multidisciplinary care environments.
Therapy Practices
Medication Management
Substance Use Treatment Providers
IOP & PHP Programs
Community Behavioral Health Organizations
Multidisciplinary Practices
Why Organizations Choose DENmaar
Technology-supported workflows backed by real reimbursement knowledge.
DENmaar combines behavioral health specialization, reimbursement research, payer insight, and operational workflow support to help organizations improve billing accuracy and financial performance.
Behavioral health specialization
Real-world payer expertise
Continuous reimbursement research
Technology-supported workflows
Shared knowledge across client organizations
Focus on reimbursement accuracy
Request an Insurance Workflow Review
Discover how DENmaar’s Insurance Knowledge Team can strengthen reimbursement operations.
Request Information
TESTIMONIALS
WHAT OUR CLIENTS SAY
On behalf of everyone at Meadowlark Counseling Services, I want to extend our sincere thanks for the continued improvements you and your team have made to the DENMaar EMR platform. We have been consistently impressed with both the functionality and user-friendly design of the system, which has made a meaningful difference in our day-to-day operations. The intuitive layout and ease of use have allowed our staff to spend less time navigating the system and more time focusing on client care. The regular updates and enhancements reflect your commitment to meeting the evolving needs of providers in the behavioral health and substance use treatment fields. We genuinely look forward to the new features introduced each month and appreciate how responsive the platform has been to the demands of clinical workflows. We have been so pleased with our experience that we’ve taken the opportunity to recommend DENMaar to other professionals in Pennsylvania who are working in the SUD field. Thank you again for your ongoing support and partnership. We are grateful to be working with a company that truly understands the needs of its users. KIndly, Becky Parks on behalf of the entire team at Meadowlark Counseling Services
I referred one of my colleagues Dr Aaron to you he is just starting g his psychology private practice and looking at where to start. I told him hands down you guys are the best billers and have a great EMR and team. He said he reached out just wanted to let you know!
FANTASTIC job keeping things rolling along with any and all of our billing concerns as well as responding to other issues which may well have been out of your wheelhouse. We are VERY grateful to have you and the crew in our corner.
I appreciate you all so much and DENmaar has been such a blessing Donna to our overall operations and success as an expanding company—allowing us to ultimately operate more efficiently, get our claims paid more consistently, ad stay on top of the critical credentialing piece, among other things. Teamwork does in fact, make the dream work. I’ll loop Chris/Isabella in on this message thread too, as I want All of your team to be aware of how much we appreciate our working relationship with DENmaar
Thank you for your diligence!! I appreciate it so much. Thank you Edwina…
Thank you so much Amy! I will be referring to DENmaar as often as I am asked about credentialing services.
Our Latest Blogs
AI Insurance Card Intelligence in Behavioral Health Billing and Revenue Cycle Management
Behavioral health revenue doesn’t break at claim submission. It breaks at intake.
The insurance ID card is the first point of truth in the revenue cycle, yet most systems treat it as a passive data entry step. In reality, this single artifact contains the routing logic that determines whether a claim gets paid or rejected.
For behavioral health practices, especially those operating across therapy, psychiatry, SUD, and higher levels of care, the complexity increases due to mental health carve-outs. These carve-outs separate behavioral health benefits from medical coverage, often assigning them to entirely different payers.
If that distinction is not identified at intake, the downstream impact is immediate: claims are sent to the wrong payer, rejected, corrected, and resubmitted, delaying revenue and increasing administrative burden.
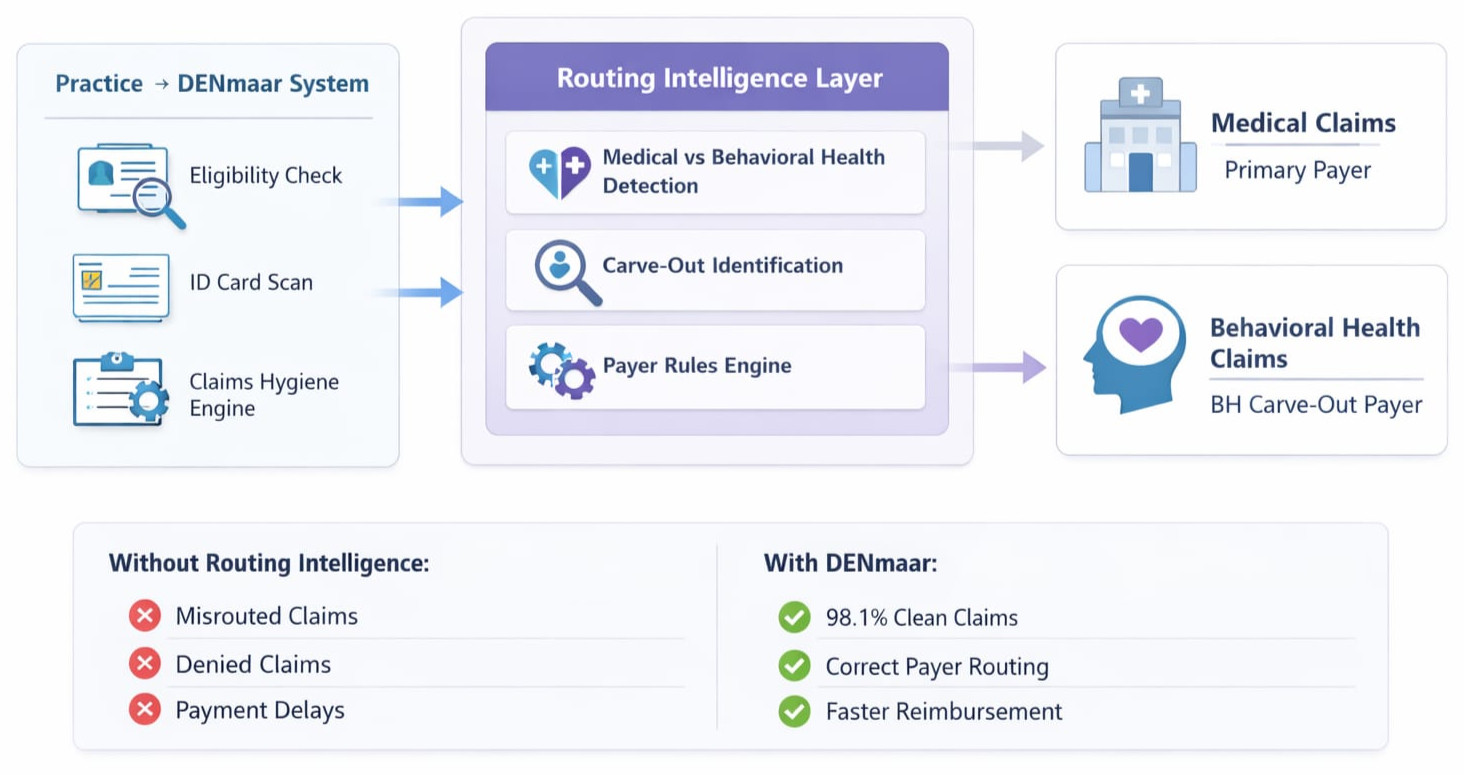
DENmaar approaches this differently by treating the ID card as a structured data source and a decision engine for payer routing.
Practices using modern behavioral health EHR systems and integrated behavioral health billing services increasingly rely on intelligent intake infrastructure to ensure payer accuracy before claims ever reach the clearinghouse.
Learn more about how preventative claims infrastructure for behavioral health billing improves revenue cycle outcomes.
The Core Problem Mental Health Carve Outs Disrupt Standard Billing Logic
Traditional EHR systems capture insurance data in flat fields: payer name, member ID, and group number. This approach assumes that the payer listed on the card is the correct destination for all services.
In behavioral health, that assumption is frequently wrong.
A single insurance card may represent:
- A medical payer such as Blue Cross Blue Shield or Aetna
- A behavioral health carve-out managed by a third party such as Carelon, Optum, or Magellan
- Separate claims addresses or submission pathways depending on service type
Without identifying these distinctions, practices unknowingly submit behavioral health claims to the medical payer. The result is predictable: rejections for incorrect payer routing.
This is not a billing issue. It is an intake intelligence issue.
You can explore how this problem affects claims performance in behavioral health billing revenue cycle failures.
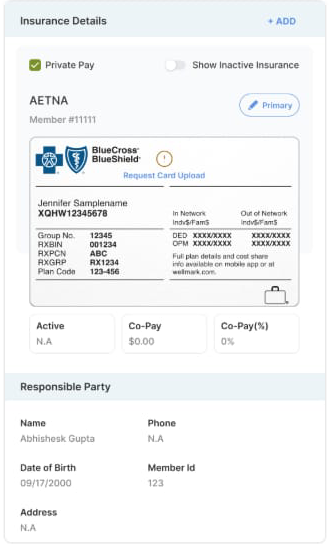
Step 1 Structured Data Extraction Not Basic OCR
Most OCR tools simply convert images into text. That is insufficient for healthcare workflows.
DENmaar’s ID card reader performs structured extraction. It identifies and categorizes specific data elements, including:
- Payer name
- Member ID
- Group number
- RX BIN, PCN, and RX Group
- Plan identifiers
- Claims submission addresses
- Network indicators
Instead of returning raw text, the system maps this information into discrete, usable data fields within the platform.
This creates a normalized dataset that can be used downstream for validation, eligibility checks, and payer routing inside a modern behavioral health EHR platform.
Learn how behavioral health EHR and mental health EHR software integrates these workflows.
Step 2 Carve Out Detection and Interpretation
The critical layer is not extraction. It is an interpretation.
DENmaar analyzes the extracted data for carve-out indicators, including:
- Keywords such as behavioral health, mental health services, or managed by
- Differences in claims addresses that suggest separate submission entities
- Plan structures tied to subcontracted behavioral health networks
- Logo and branding recognition that signal payer relationships
Based on these signals, the system determines whether behavioral health services should be routed to a different payer than the one prominently displayed on the card.
The output is not just a flag, but a routing recommendation embedded into the workflow.
This intelligence contributes to stronger clean claims performance in behavioral health revenue cycle management.
See how this connects to claims hygiene in behavioral health billing.
Step 3 Real Time Payer Routing Within the Workflow
Once a carve-out is detected, that intelligence is applied across the entire revenue cycle.
At the scheduling level, the system associates the correct payer with the appointment based on service type. Therapy, medication management, and higher levels of care can each trigger different routing logic.
At the documentation level, diagnoses and service codes are validated against the expected payer structure to ensure consistency.
AI driven documentation systems also help standardize billing alignment through AI documentation for behavioral health and AI progress notes.
At the daysheet level, where claims are finalized, the system enforces the correct payer destination before submission.
This eliminates one of the most common sources of claim rejection: sending claims to the wrong payer.
Step 4 Alignment with Eligibility and Authorization
Correct payer identification at intake ensures that all subsequent processes are aligned.
Eligibility checks are performed against the appropriate behavioral health payer rather than the medical plan.
Authorization requirements are tracked under the correct entity, preventing mismatches between approved services and submitted claims.
Patient responsibility calculations, including copays and coinsurance, reflect the actual behavioral health benefits rather than generalized medical coverage.
This is particularly important for Medicaid billing behavioral health, psychiatry billing Medicaid, and substance use treatment billing, where carve-outs are common and rules are highly specific.
Organizations managing these workflows often combine EHR infrastructure with behavioral health billing services and mental health billing services.
Step 5 Continuous Learning through Claim Outcomes
DENmaar’s system does not rely solely on static rules. It incorporates feedback from real claim outcomes.
When a claim is rejected due to incorrect payer routing, that data is captured and used to refine future routing decisions.
When a claim is successfully processed and paid, it reinforces the accuracy of the existing logic.
Over time, this creates a continuously improving payer intelligence layer that adapts to real-world variations across plans and regions.
This adaptive intelligence is a core component of RCM for behavioral health and clean claims optimization.
More about the platform approach can be found at:
www.denmaar.com
Financial Impact Why Accurate Payer Routing Matters
Accurate payer routing at intake has a direct and measurable impact on revenue performance.
Practices using an integrated system like DENmaar typically experience:
- A 10 to 20 percent increase in insurance revenue
- Significantly higher clean claim rates
- Reduced administrative time spent on corrections and resubmissions
- Faster reimbursement cycles
These outcomes are not driven by post submission follow up. They are achieved by preventing errors before the claim is ever created.
The Intake to Claim Flywheel
DENmaar’s ID card reader is not an isolated feature. It is the entry point into a larger system designed to optimize claims performance.
The workflow operates as a continuous cycle:
- ID card capture and structured extraction
- Carve out detection and payer interpretation
- Eligibility and authorization alignment
- Scheduler, documentation, and daysheet enforcement
- Clean claim submission
- Feedback loop from claim outcomes
By embedding intelligence at the very beginning of the process, the system ensures that every downstream step operates with accurate, actionable data.
Conclusion
Most systems treat the insurance card as a static input. DENmaar treats it as a dynamic source of payer logic.
By extracting, interpreting, and operationalizing the information contained on the card, the platform ensures that behavioral health claims are routed correctly before submission.
This approach transforms intake from a clerical task into a core component of revenue optimization.
DENmaar does not just read insurance cards. It interprets payer logic in real time, ensuring that every behavioral health claim is sent to the right payer from the start.
Frequently Asked Questions
Why are mental health carve outs important in behavioral health billing?
Mental health carve outs separate behavioral health benefits from medical insurance coverage. If a practice submits claims to the medical payer instead of the behavioral health payer, the claim is often rejected. Correct carve out detection ensures accurate payer routing and higher clean claim rates.
How does AI improve behavioral health revenue cycle management?
AI improves behavioral health revenue cycle management by analyzing payer rules, validating documentation, detecting billing inconsistencies, and ensuring claims are routed to the correct payer before submission.
What is the role of an insurance card reader in behavioral health billing?
An AI insurance card reader extracts structured payer data from insurance cards, detects behavioral health carve outs, and ensures claims are routed correctly. This reduces administrative work and improves Medicaid behavioral health reimbursement.
Why do behavioral health claims get rejected due to payer routing?
Claims are often rejected when the payer responsible for behavioral health services differs from the medical payer on the card. Without carve out detection and payer intelligence, claims may be submitted to the wrong payer.
AI in Behavioral Health Billing: Beyond the Buzzwords
Turning Complex Care into Clean, Payable Claims
Artificial Intelligence is everywhere in healthcare right now.
But most of it is noise.
Chatbots. Auto notes. Surface level automation.
None of that solves the real problem behavioral health practices face:
How do you consistently turn complex, multidisciplinary care into clean, payable claims?
That is where AI actually matters.
Modern behavioral health EHR systems and behavioral health revenue cycle management platforms must focus on turning documentation into compliant claims that meet payer rules, Medicaid billing requirements, and behavioral health compliance standards.
The Real Use Case: Claims Intelligence, Not AI Features
AI is not most valuable in generating notes or answering phones.
It is most valuable when it acts as a real time enforcement and learning layer across your behavioral health revenue cycle management workflow.
Specifically:
- Before submission ensuring claims are correct
- After submission ensuring revenue is optimized
Everything else is secondary.
Systems that integrate behavioral health billing services, documentation, and payer rules directly into a unified platform like behavioral health EHR and mental health EHR software can dramatically improve claims accuracy and reimbursement performance.
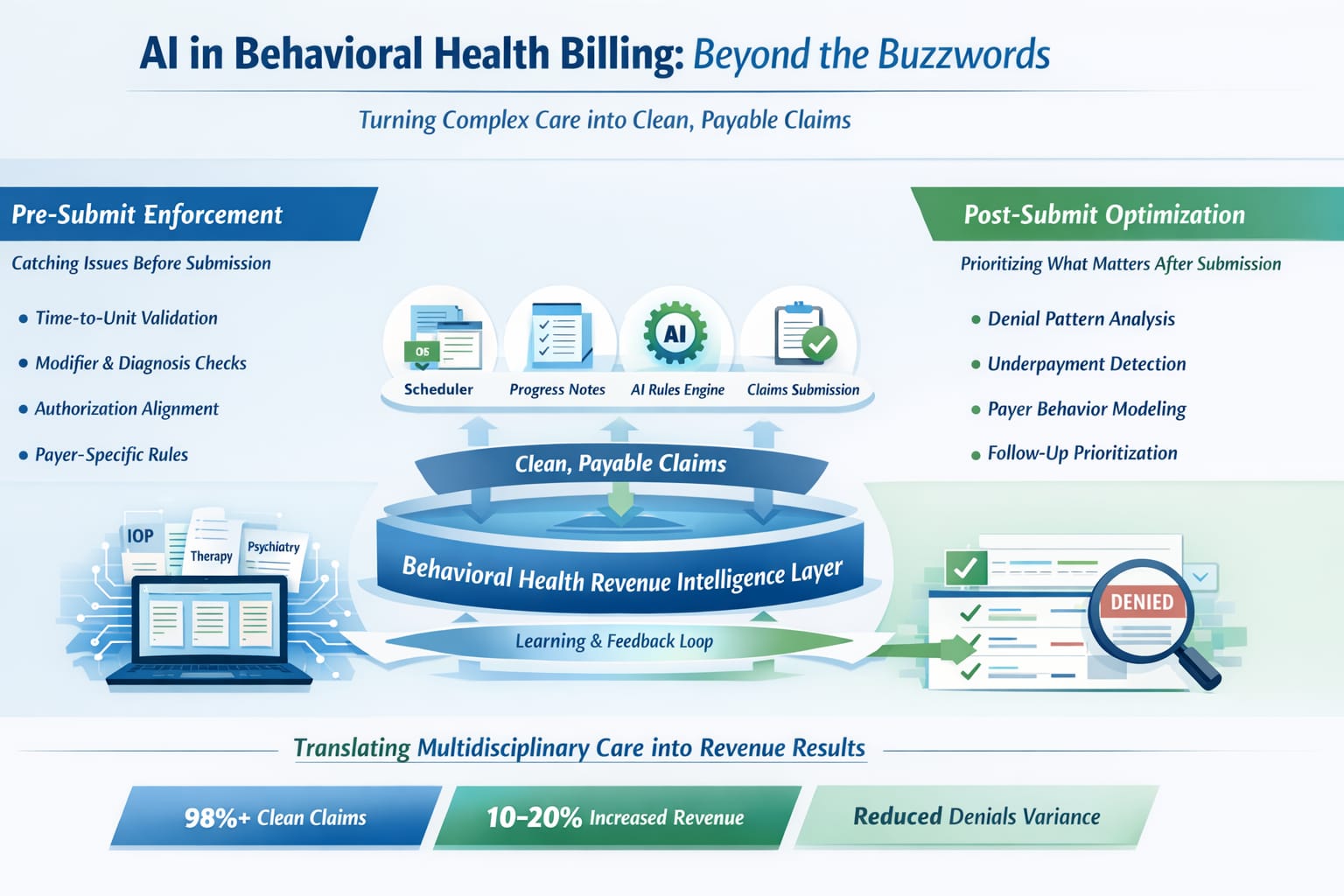
1. Pre Submit: Where Revenue Is Won or Lost
Most revenue leakage happens before a claim is ever submitted.
Not because providers are not doing the work but because:
- Rules vary by payer
- Documentation does not map cleanly to billing
- Multidisciplinary workflows create inconsistencies
This is where AI delivers the highest ROI.
What AI Should Be Doing Pre Submit
A true system should function as a claims hygiene engine, enforcing standards across the behavioral health billing workflow.
Learn more about building claims hygiene in behavioral health billing.
- Time to Unit Validation
Ensuring session duration aligns with CPT codes such as 90837 vs 90834.
- Modifier Logic
Applying correct modifiers like 59 or XE based on context.
- Diagnosis to Service Alignment
Not just valid but likely to pay.
- Authorization Tracking
Matching authorized units to scheduled and documented services.
- Place of Service Accuracy
Telehealth versus in person versus facility based services mapped correctly per payer.
- UB04 vs CMS 1500 Routing
Determining the correct billing form based on service type, payer requirements, and facility structure.
This distinction between CMS 1500 vs UB 04 billing models is critical for organizations handling therapy, psychiatry, and facility services.
The Key Insight
This is not about replacing rules.
It is about managing rule complexity at scale across:
- Multiple disciplines
- Multiple payers
- Multiple program types
Organizations that invest in modern RCM for behavioral health infrastructure can dramatically reduce billing friction and increase Medicaid behavioral health reimbursement accuracy.
2. The Hidden Problem: Multidisciplinary Complexity
Most systems are built for one type of provider.
Behavioral health is not.
You are managing:
- Therapy
- Psychiatry
- Case management
- SUD, IOP, and facility services
Each with:
- Different documentation
- Different billing rules
- Different compliance requirements
Where AI Actually Wins
AI creates a translation layer between:
What happened clinically
What is billable
What will get paid
This is where most revenue is lost and where most systems fail.
Platforms that integrate documentation with billing such as AI powered progress notes for behavioral health help ensure clinical documentation aligns with payer requirements and CPT coding rules.
3. Post Submit: Where AI Becomes a Force Multiplier
Once claims are submitted, the problem changes.
Now it is not about correctness. It is about optimization.
What AI Should Be Doing Post Submit
- Denial Pattern Analysis
Identifying systemic issues instead of isolated denials. - Payer Behavior Modeling
Understanding which payers delay, deny, or underpay. - Follow Up Prioritization
Directing billing teams toward tasks that actually drive ROI. - Underpayment Detection
Comparing expected versus actual reimbursement across Medicaid, commercial payers, and facility claims.
Practices that use specialized behavioral health billing services integrated with AI systems gain far more visibility into payer performance and reimbursement trends.
Important Distinction
AI should not replace your billing team.
It should make your billing team exponentially more effective.
Modern therapy practice management software and mental health EHR systems should combine automation with human expertise to strengthen the behavioral health revenue cycle.
4. What AI Is NOT Good At
To be clear, there are areas where AI is overhyped:
- Fully autonomous payer calls
- Portal scraping at scale
- Static rule engines
- Generic note generation disconnected from billing
These approaches do not reduce denials.
They often increase them.
This is why many practices struggle when their technology stack separates documentation, billing, and revenue cycle management, a challenge explored in why many behavioral health EHR billing systems fail.
5. The Architecture That Actually Works
The future is not ‘AI tools’.
It is an integrated system:
- Scheduler
Sets expected billing reality. - Progress Notes
Confirm clinical and compliance reality. - Daysheet (Critical Layer)
AI answers:
Can this be billed?
Will this get paid?
- Claim Submission
Clean validated output. - Post Submit Engine
Learns → feeds back → improves system
This approach is known as preventative claims infrastructure, which focuses on preventing denials before they occur rather than fixing them later.
You can explore the full model of preventative claims infrastructure for behavioral health billing.
6. The Outcome: Measurable, Not Theoretical
When implemented correctly:
- 98% + clean claims
- Reduced denial variability across disciplines
- Faster onboarding of complex practices
- Less dependency on highly specialized billing staff
And most importantly:
A 10 to 20% increase in insurance revenue
Not by charging more.
But by capturing revenue that was already being earned and lost in complexity.
Organizations using integrated behavioral health revenue cycle management systems consistently outperform fragmented technology stacks.
Final Thought
AI in behavioral health is not about automation.
It is about enforcement and translation.
Turning multidisciplinary care into structured, compliant, payable claims every time.
That is where the real value is.
At DENmaar, this intelligence is built directly into the platform where documentation, billing, and claims performance function as a single unified system.
Because in behavioral health, revenue does not break at billing.
It breaks upstream.
Frequently Asked Questions
How does AI improve behavioral health billing?
AI improves behavioral health billing by validating CPT codes, modifiers, diagnosis alignment, and authorization requirements before claims are submitted. This increases clean claim rates and reduces denials.
What is claims hygiene in behavioral health billing?
Claims hygiene refers to validating documentation, coding, payer rules, and billing requirements before claim submission to ensure claims are accurate and payable.
Can AI help with Medicaid behavioral health billing?
Yes. AI systems can help verify eligibility, ensure correct CPT coding, validate CMS 1500 vs UB 04 claim routing, and improve Medicaid reimbursement accuracy.
What role does an EHR play in behavioral health revenue cycle management?
A modern behavioral health EHR integrates documentation, coding, and billing workflows to ensure clinical care translates directly into compliant claims.
What are clean claims in behavioral health billing?
Clean claims are insurance claims that pass payer validation without errors, reducing rejections and speeding up reimbursement.
The System Is Broken Because It Fixes Problems Too Late
There’s a fundamental flaw in how behavioral health billing systems are designed.
And most people don’t question it.
The entire model, including EHR platforms, billing companies, and clearinghouses, is built around one assumption:
Submit the claim first. Fix the problem later.
That approach has shaped the entire behavioral health revenue cycle management system.
But it is also the reason many practices quietly lose revenue.
The Hidden Cost of Fixing It Later
On paper, it works.
In reality, it creates:
- Denials
- Delays
- Rework
- Cash flow instability
A claim gets submitted. It gets rejected. Someone reviews it. Fixes it. Resubmits it. Waits again.
Multiply that across hundreds or thousands of claims per month and you get a system that quietly bleeds revenue.
Not because providers are doing anything wrong but because the system is designed to catch errors after they happen.
Many organizations do not realize they are experiencing the same structural problem described in why behavioral health practices lose 10–20 percent of insurance revenue due to inefficient claims workflows and billing friction.
The Problem Is Not Billing. It Is Timing
Most platforms focus on documentation.
Most billing teams focus on follow up.
Very few systems focus on the moment that actually matters.
Before the claim is created.
That is where revenue is won or lost.
Modern systems designed for behavioral health practices integrate clinical documentation and billing logic within a behavioral health EHR and mental health practice management platform so that claims data is structured correctly from the beginning.
A Different Approach: Preventative Claims Infrastructure
At DENmaar, we have taken a different position.
We do not believe in submitting claims and hoping they go through.
We believe:
If a claim is not clean, it should not exist.
This philosophy is built around clean claims infrastructure and behavioral health billing accuracy, which significantly improves Medicaid behavioral health reimbursement and insurance claim approval rates.
What That Looks Like in Practice
Before a claim is ever submitted, the system should:
- Verify insurance and payer routing
- Confirm provider credentialing
- Validate CPT and diagnosis alignment
- Check authorization requirements
- Flag modifier and place of service issues
Only then should a claim be released.
Not after a denial. Not after a delay.
Before.
Maintaining strong claims hygiene in behavioral health billing ensures that payer data, coding accuracy, and provider credentials are verified before submission.
That proactive model eliminates much of the friction that typically slows Medicaid claims for behavioral health providers.
Why This Matters Now
In today’s environment, practices do not just need growth.
They need:
- Predictable cash flow
- Fewer administrative headaches
- Confidence in their revenue cycle
A reactive system cannot provide that.
A preventative system can.
Organizations increasingly rely on specialized behavioral health billing services and revenue cycle management that prioritize claim accuracy before submission rather than correction after denial.
The Result
When you shift from reactive to preventative:
- Denials decrease
- Payments accelerate
- Teams spend less time fixing errors
- Revenue becomes more predictable
Practices typically see a 10–20 percent increase in insurance revenue not because they are doing more work but because they are eliminating friction within the behavioral health billing process.
Why Our Model Is Different
Most platforms charge a monthly subscription.
Most billing companies charge for activity whether the system is efficient or not.
We do not.
At DENmaar behavioral health EHR and revenue cycle platform, incentives are aligned directly with outcomes.
We invoice based on claims performance.
That means:
- If claims are cleaner revenue improves
- If revenue improves we grow with you
Our incentives are tied to one thing.
Getting claims right the first time.
Not generating more work. Not fixing avoidable errors.
Integrated documentation workflows including AI progress notes for behavioral health documentation help ensure clinical records support both care quality and billing compliance.
This Is Not an Upgrade. It Is a Different System
We are not trying to make billing more efficient.
We are redefining when and how billing decisions happen.
The traditional model says:
Submit then fix later.
We believe:
Fix first. Submit once. Get paid.
This preventative infrastructure model represents the future of behavioral health revenue cycle management and Medicaid billing optimization.
Final Thought
If your current system depends on catching mistakes after the fact, it is not optimized. It is reactive.
And in a system as complex as behavioral health billing, reactive systems are expensive.
The future is not faster billing.
It is cleaner claims from the start.
Frequently Asked Questions
What is preventative claims infrastructure in behavioral health billing?
Preventative claims infrastructure focuses on identifying billing errors before claims are submitted. This includes verifying insurance eligibility, provider credentialing, coding alignment, and authorization requirements to ensure clean claims.
Why do behavioral health claims get denied?
Common reasons include incorrect modifiers, incomplete documentation, missing authorizations, eligibility verification errors, and incorrect claim types such as CMS-1500 vs UB-04.
How does clean claims infrastructure improve Medicaid behavioral health reimbursement?
Clean claims reduce rejections and denials, allowing claims to move through payer systems faster. This leads to faster reimbursements, improved cash flow, and fewer administrative corrections.
Can AI help improve behavioral health billing accuracy?
Yes. AI tools can generate structured documentation, validate billing requirements during clinical workflows, and improve data integrity for claims submission. This reduces coding errors and improves billing compliance.
Our Partners
Ready to get started?
Feel free to reach out if you have any questions.