- Respond to callers when staff are busy or unavailable
- Reduce missed opportunities from after-hours and weekend calls
- Provide a more consistent intake and scheduling experience
- Keep communication workflows moving without depending on office hours alone
AI RECEPTIONIST FOR BEHAVIORAL HEALTH
Never Miss a Call, Intake
Opportunity, or Scheduling
Request.
Behavioral health practices lose potential clients every day because calls go
unanswered, staff are busy, or intake requests arrive after hours. DENmaar AI
Receptionist helps practices capture opportunities, improve responsiveness,
and reduce administrative workload.
Immediate Call Response
Behavioral Health Workflows
Integrated Scheduling & Intake
Supported functions include
Built for Behavioral Health Organizations
Unlike generic answering services, DENmaar AI Receptionist is designed specifically for behavioral
health workflows and patient communication needs.
01
New patient intake
Capture initial caller details and support first-contact intake workflows for prospective patients.
02
Appointment Scheduling
Help callers request available appointments and move scheduling requests into the right workflow.
03
Appointment Rescheduling
Support reschedule requests without requiring every call to be handled directly by staff.
04
Frequently Asked Questions
Provide helpful responses to common patient questions about practice operations, locations, or services.
05
Insurance Intake Collection
Collect insurance-related details needed for intake workflows and claims readiness preparation.
06
Message Routing
Route messages and requests to the appropriate team, department, or follow-up queue.
07
After-Hours Call Handling
Respond to callers outside business hours so opportunities are not lost overnight or on weekends.
08
Call Summaries
Provide staff with a concise summary of the call, captured details, and recommended next steps.
09
Provider & Location Routing
Direct patients to the right provider, office, or service line based on their needs and request type.
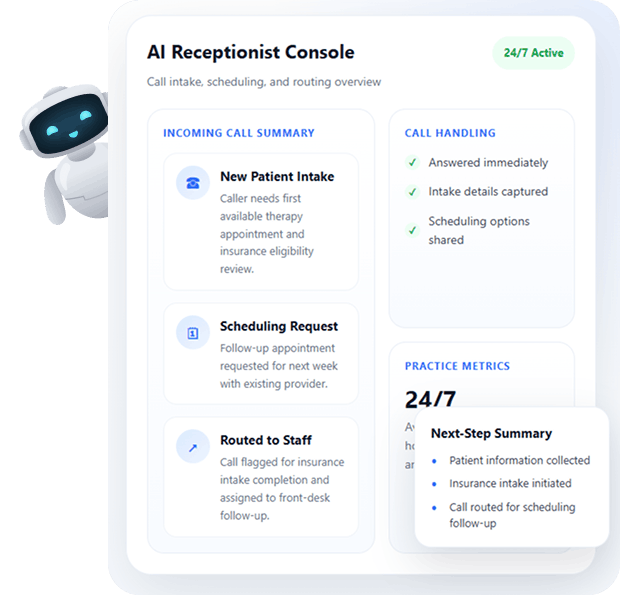
HOW IT WORKS
From Incoming Call to Actionable Next Step
AI Receptionist helps practices respond quickly, collect the right information, and move requests into
scheduling, routing, or follow-up workflows.
Patient calls your practice
AI Receptionist answers immediately
Information is collected and documented
Calls are routed, scheduled, or assigned for follow-up
Staff receive a summary and next steps
AVAILABLE 24/7
Support Call Handling During Business Hours, Evenings, Weekends, and Holidays
The AI Receptionist can answer calls during business hours, evenings, weekends, and holidays, helping ensure every caller receives a professional response and every opportunity has a better chance of being captured.
Coverage Overview
24/7 Support
Business Hours
Support routine call handling, intake questions, and appointment scheduling requests during the workday.
Evenings
Respond to callers outside traditional office hours when prospective patients are often more available.
Weekends
Capture new opportunities and requests that might otherwise wait until Monday or go unanswered.
Holidays
Maintain a professional first response experience even when the office is closed or staff availability is limited.
INTEGRATED WITH THE DENMAAR PLATFORM
Integrated with the DENmaar Platform
Documentation can connect directly to scheduling, treatment plans, assessments, billing workflows,
claims validation, and provider productivity reporting.
Scheduling
Patient Registration
Insurance Intake
DENmaar AI
Receptionist
Receptionist
Documentation Workflows
Billing Operations
Provider Assignments
WHY ORGANIZATIONS CHOOSE DENMAAR
Built to Improve Responsiveness, Reduce Workload, and Support Better Intake Operations
DENmaar AI Receptionist is designed to help behavioral health organizations respond faster, route requests more effectively, and reduce front-desk strain.
- Immediate Call Response
- Reduced Front Desk Workload
- Improved Patient Experience
- Better Intake Consistency
- Behavioral Health Focused Workflows
- Fully Integrated Platform
Request an
AI Receptionist Demo
Experience how DENmaar AI Receptionist can help your organization capture more opportunities,
- Improve responsiveness
- Streamline intake operations.
Request Information
TESTIMONIALS
WHAT OUR CLIENTS SAY
On behalf of everyone at Meadowlark Counseling Services, I want to extend our sincere thanks for the continued improvements you and your team have made to the DENMaar EMR platform. We have been consistently impressed with both the functionality and user-friendly design of the system, which has made a meaningful difference in our day-to-day operations. The intuitive layout and ease of use have allowed our staff to spend less time navigating the system and more time focusing on client care. The regular updates and enhancements reflect your commitment to meeting the evolving needs of providers in the behavioral health and substance use treatment fields. We genuinely look forward to the new features introduced each month and appreciate how responsive the platform has been to the demands of clinical workflows. We have been so pleased with our experience that we’ve taken the opportunity to recommend DENMaar to other professionals in Pennsylvania who are working in the SUD field. Thank you again for your ongoing support and partnership. We are grateful to be working with a company that truly understands the needs of its users. KIndly, Becky Parks on behalf of the entire team at Meadowlark Counseling Services
I referred one of my colleagues Dr Aaron to you he is just starting g his psychology private practice and looking at where to start. I told him hands down you guys are the best billers and have a great EMR and team. He said he reached out just wanted to let you know!
FANTASTIC job keeping things rolling along with any and all of our billing concerns as well as responding to other issues which may well have been out of your wheelhouse. We are VERY grateful to have you and the crew in our corner.
I appreciate you all so much and DENmaar has been such a blessing Donna to our overall operations and success as an expanding company—allowing us to ultimately operate more efficiently, get our claims paid more consistently, ad stay on top of the critical credentialing piece, among other things. Teamwork does in fact, make the dream work. I’ll loop Chris/Isabella in on this message thread too, as I want All of your team to be aware of how much we appreciate our working relationship with DENmaar
Thank you for your diligence!! I appreciate it so much. Thank you Edwina…
Thank you so much Amy! I will be referring to DENmaar as often as I am asked about credentialing services.
Our Latest Blogs

Why Behavioral Health Needs a New Operating Model
Multidisciplinary Care, Dual Claim Systems, and the Rise of Claims Hygiene
Behavioral health is changing.
Over the past decade, the industry has expanded beyond traditional outpatient therapy into a much broader continuum of care. Today’s practices increasingly include multiple service lines:
- Outpatient therapy
- Psychiatry and medication management
- Substance use disorder (SUD) treatment
- Intensive outpatient programs (IOP)
- Partial hospitalization programs (PHP)
- Community-based services
- Residential programs such as ASAM 3.1
Yet the technology supporting many of these organizations still assumes a simple model: one provider, one discipline, one claim type.
That assumption no longer holds.
Modern behavioral health organizations require systems designed around multiple disciplines, multiple billing frameworks, and increasingly complex payer rules.
The practices that understand this shift are building something fundamentally different.
For many organizations, adopting a modern behavioral health EHR platform and integrated behavioral health revenue cycle management approach is the first step toward solving these challenges.
The Multidisciplinary Behavioral Health Organization
The most resilient behavioral health organizations today are not single-service clinics.
They are multidisciplinary systems of care.
A single organization might include:
- Licensed therapists
- Psychiatrists and psychiatric nurse practitioners
- SUD counselors
- Case managers
- Community support specialists
- Residential program staff
Each discipline introduces different documentation standards, payer expectations, and billing structures.
A therapy session may be billed as CPT 90837, while case management could use T1016, and an intensive outpatient day might involve a facility-based service with entirely different billing rules.
Trying to run this ecosystem on software designed only for therapy quickly creates friction.
This is where the distinction between professional claims and facility claims becomes critical.
Many organizations discover they are losing significant insurance revenue due to billing inefficiencies, something explored in detail in this analysis of how providers lose 10–20% of insurance revenue due to revenue cycle gaps.
CMS-1500 vs UB-04: Two Claim Worlds in Behavioral Health
Behavioral health providers often operate across two fundamentally different claim systems.
Understanding CMS 1500 vs UB 04 billing is essential for accurate Medicaid behavioral health reimbursement and clean claims.
CMS-1500 (Professional Claims)
Used for services delivered by individual clinicians such as:
- Therapy sessions
- Psychiatric evaluations
- Medication management
- Individual counseling
These claims are built around:
- CPT / HCPCS procedure codes
- Rendering provider information
- Service units and modifiers
This is the traditional model most EHRs support.
But it is only half the story.
UB-04 (Facility Claims)
Programs such as IOP, PHP, residential treatment, and some SUD services may require facility billing.
These claims rely on a completely different structure:
- Revenue codes
- Facility identifiers
- Program-level billing logic
- Episode-based service tracking
Many organizations running these services discover that their EHR cannot properly support UB-04 workflows.
As a result, staff often build manual workarounds, spreadsheets, and external billing processes.
The operational cost of this fragmentation is enormous.
This is why many providers adopt specialized behavioral health billing services designed for complex Medicaid and multi-program organizations.
The Hidden Problem: Claims Hygiene in Behavioral Health Billing
Even with the right claim format, most behavioral health revenue cycles struggle with something far more basic.
Data integrity.
We call this claims hygiene in behavioral health billing.
Claims hygiene refers to the accuracy and completeness of the information required to produce a clean claim:
- Correct insurance identification
- Accurate payer routing
- Valid provider credentials
- Proper service coding
- Diagnosis linkage
- Authorization verification
- Clean eligibility data
When these elements are wrong or incomplete, claims fail.
The result is familiar to many organizations:
- Rising denial rates
- Aging receivables
- Administrative overload
- Lost revenue
Improving claims hygiene is often the fastest way to increase revenue without seeing a single additional patient.
Where Most Behavioral Health Systems Fail
Many EHR platforms were originally designed for small outpatient therapy practices.
They assume a simple model:
One clinician
One note
One claim
But multidisciplinary behavioral health organizations operate in a very different reality.
They need systems capable of supporting:
- Multiple clinical disciplines
- CMS-1500 professional claims
- UB-04 facility claims
- Complex Medicaid program structures
- Integrated behavioral health revenue cycle management workflows
Without this architecture, billing becomes an afterthought rather than an integrated system.
Organizations increasingly turn to purpose-built platforms like DENmaar EHR, designed specifically for behavioral health compliance, Medicaid billing workflows, and multi-program organizations.
The Future: Integrated Behavioral Health Operating Systems
The next generation of behavioral health platforms will not separate clinical documentation from revenue cycle management.
Instead, they will treat documentation, scheduling, and billing as a single operational system.
This means:
- Services mapped to claim type (CMS-1500 or UB-04)
- Documentation structured to support billing requirements
- Eligibility and payer data captured early in the workflow
- Claims validated before submission
When this approach is implemented correctly, organizations see dramatic improvements:
- Higher clean claim rates
- Faster reimbursements
- Reduced administrative workload
- More predictable revenue
Modern platforms are also introducing AI progress notes for behavioral health, allowing clinicians to automate documentation while maintaining compliance with billing requirements.
A System Designed for the Real Behavioral Health Market
The behavioral health industry is not simple.
It spans therapy, psychiatry, substance use treatment, residential care, and community-based services.
Technology must reflect that complexity.
The organizations that thrive in the next decade will be those that build systems around three principles:
- Multidisciplinary care delivery
- Support for both CMS-1500 and UB-04 claim structures
- Operational discipline around claims hygiene
This is not just a billing strategy.
It is a new operating model for behavioral health.
Frequently Asked Questions
What is the difference between CMS-1500 and UB-04 in behavioral health billing?
CMS-1500 is used for professional claims submitted by individual providers such as therapists and psychiatrists. UB-04 is used for facility-based services like intensive outpatient programs, residential treatment, and hospital services.
Why is claims hygiene important in behavioral health revenue cycle management?
Claims hygiene ensures that all billing data such as insurance information, provider credentials, and service codes are accurate before submission. Strong claims hygiene improves clean claims rates, Medicaid reimbursement, and behavioral health revenue cycle performance.
What software do behavioral health organizations need?
Modern organizations require behavioral health EHR systems with integrated billing, Medicaid claims support, and AI documentation tools to manage multidisciplinary care and complex billing workflows.
How can AI help behavioral health documentation?
AI documentation tools can generate AI progress notes and clinical summaries, reducing clinician workload while ensuring notes meet compliance and billing requirements.
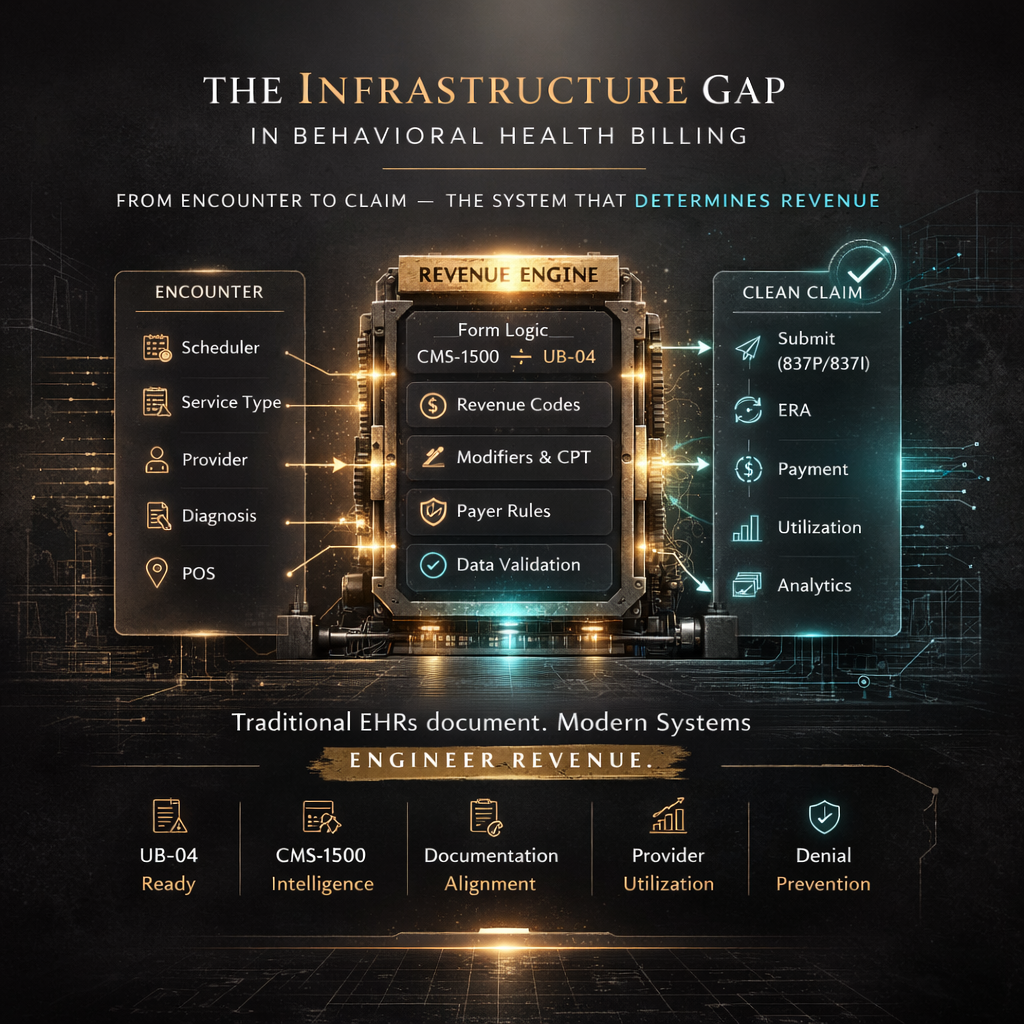
The Infrastructure Gap in Behavioral Health Billing
Why most EHR platforms were never designed for complex revenue
Behavioral health has a revenue problem and it isn’t payer rates.
It’s infrastructure.
Most EHR platforms were designed for documentation first, billing second. That model works for solo therapy practices submitting basic CMS-1500 claims. It breaks down the moment complexity enters the picture.
And complexity is now the rule, not the exception.
For many organizations, this structural gap is one of the reasons behavioral health practices lose 10–20% of insurance revenue without realizing it.
Where Systems Begin to Fail
As practices expand into:
- Intensive Outpatient Programs (IOP)
- Community Mental Health (CMHC) services
- ACT, PSR, and H2038 programs
- Multi-discipline care models
- Medicaid Managed Care carve-outs
They encounter a structural reality:
CMS-1500 logic alone is not enough.
UB-04 becomes necessary. Revenue codes become necessary. Type-of-Bill fields matter. Rendering vs. attending provider logic matters. Diagnosis pointers and modifiers are no longer optional details — they are claim survival requirements.
Yet most platforms treat these as add-ons, not core architecture.
That’s the gap.
Without strong behavioral health billing services and revenue cycle management infrastructure, these requirements create systemic claim friction.
The Encounter to Claim Disconnect
In many systems:
Scheduler → Note → Claim
are loosely connected.
But in complex billing environments, these must be unified.
At the encounter level, the system must already know:
- Whether the service maps to CMS-1500 or UB-04
- What revenue code is required
- What modifiers are payer-specific
- Which provider field populates where
- How diagnosis pointers align to CPT lines
- What place of service logic applies
If this logic is not embedded upstream, denial management becomes downstream chaos.
Strong behavioral health EHR and mental health EHR software must align documentation, billing rules, and payer requirements before a claim is generated.
Clean Claims Are an Architectural Outcome
High clean-claim rates are not achieved by working harder.
They are achieved by designing systems where:
- Documentation aligns with billing requirements
- Service types control form type automatically
- Revenue codes are required when necessary
- Payer rule tables are embedded
- Eligibility carve-outs are detected before submission
This approach reflects the concept of claims hygiene in behavioral health billing, where payer rules and documentation logic are enforced upstream.
When infrastructure is correct, denials decline structurally.
When infrastructure is weak, billing teams become firefighters.
Utilization Is Revenue, Not Just Scheduling
A second infrastructure blind spot is provider utilization.
Behavioral health revenue is directly tied to:
- Delivered units
- Authorization alignment
- Cancellation management
- Provider productivity
If your system cannot measure utilization accurately, it cannot optimize revenue.
In percentage-based revenue models, this alignment becomes even more critical.
Structured clinical documentation, including AI-assisted progress notes for behavioral health, can also support payer-aligned billing accuracy and improve clean claims performance.
The Shift That’s Coming
The era of disconnected tools is fading.
Documentation, billing logic, and utilization reporting must converge into a single revenue-intelligent engine.
Behavioral health is becoming more complex, not less. Medicaid programs are expanding. Multi-discipline care models are growing. Compliance scrutiny is increasing.
Infrastructure must mature accordingly.
The practices that win over the next decade will not simply document well.
They will design their revenue systems deliberately.
Organizations building scalable behavioral health infrastructure increasingly rely on integrated systems such as DENmaar’s behavioral health platform.
No hype.
No promises.
Just structural clarity.
Frequently Asked Questions
Why do many behavioral health EHR systems struggle with complex billing?
Many EHR platforms were originally designed for documentation rather than revenue cycle management. When organizations add services like IOP, CMHC programs, or Medicaid-based care, the billing complexity exceeds the system’s original architecture.
What is the difference between CMS-1500 and UB-04 billing in behavioral health?
CMS-1500 forms are typically used for professional services such as therapy and psychiatry. UB-04 forms are used for institutional services such as IOP or facility-based care where revenue codes and type-of-bill fields are required.
What is behavioral health claims hygiene?
Claims hygiene refers to structuring documentation, payer logic, eligibility verification, and billing rules so that claims are correct before submission, reducing denials and improving clean claim rates.
Why is revenue cycle infrastructure important for Medicaid behavioral health billing?
Medicaid behavioral health programs often include carve-outs, unique modifiers, HCPCS codes, and authorization rules. Without integrated infrastructure inside the EHR and billing workflow, practices experience denials, delays, and revenue leakage.
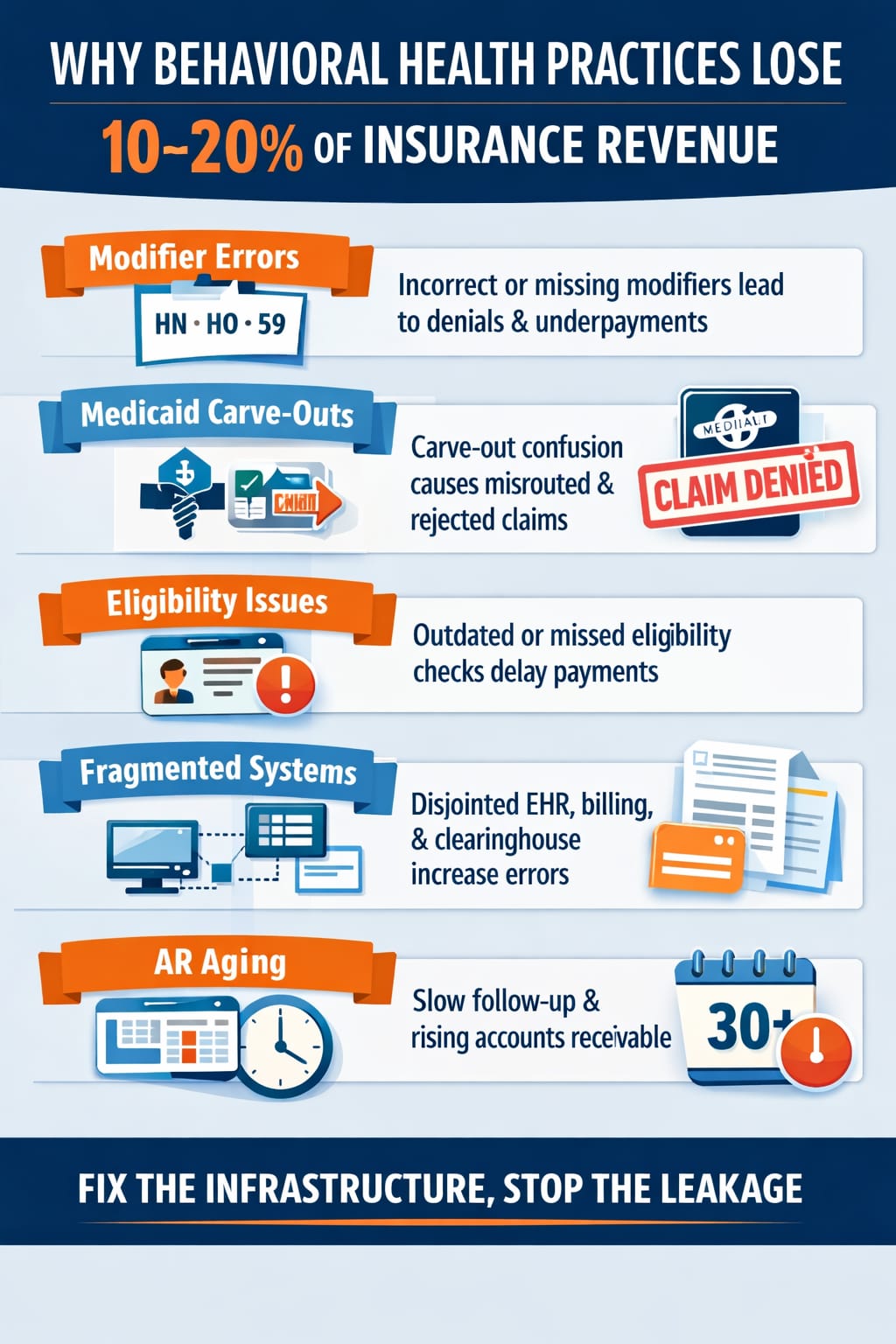
Why Behavioral Health Practices Lose 10 to 20 Percent of Insurance Revenue Without Realizing It
Most behavioral health practices believe their billing is “fine.”
Claims are going out. Payments are coming in. Denials do not look catastrophic.
But here is the uncomfortable reality:
Many practices quietly lose 10 to 20 percent of their insurance revenue, not because of fraud, incompetence, or bad providers, but because of structural claims friction.
Let’s break down where it actually leaks.
For a deeper system-level explanation, see claims hygiene in behavioral health billing.
1. Modifier Misalignment
Behavioral health is modifier heavy:
- HN / HO / HQ / HR
- 59 vs XE
- Facility vs professional billing logic
- State specific Medicaid rules
If modifier logic is not system enforced before submission, denials increase or worse, underpayments go unnoticed.
Small errors multiplied across thousands of Medicaid claims behavioral health submissions equal real revenue loss.
Without integrated behavioral health billing services and structured validation inside the EHR, modifier drift becomes systemic.
2. Medicaid Carve-Out Confusion
Behavioral health is often carved out from:
- Standard MCOs
- Commercial BCBS products
- State Medicaid networks
If eligibility verification does not detect carve-outs correctly, claims get routed incorrectly or denied after 30 or more days.
That is not a provider problem. That is infrastructure failure.
Strong behavioral health EHR and mental health EHR software systems must detect payer carve-outs before claims are generated.
3. Eligibility Gaps
Manual eligibility checks miss:
- Coverage changes
- Terminations
- Plan transitions
- Secondary payer coordination
A single eligibility miss can delay payment 45 to 60 days.
Multiply that across 15 to 20 providers and AR silently stretches.
Effective RCM for behavioral health requires real time eligibility logic built directly into the workflow, not spreadsheet tracking.
4. Fragmented Tools
Most practices operate with:
- Standalone EHR
- External biller
- Clearinghouse
- Manual tracking spreadsheets
- Email based follow up
Every handoff increases error probability.
Disconnected systems create invisible friction.
Integrated infrastructure, where EHR, documentation, and revenue cycle management operate together, reduces that friction significantly.
See how a technology plus services model works in practice
5. AR Aging Without Automation
If 30 day AR is not aggressively monitored and worked:
Revenue decays.
Most billing teams are reactive.
Top performing behavioral health revenue cycle management systems are proactive.
When claims infrastructure is engineered upstream, including structured documentation such as AI powered progress notes that align with payer rules, AR stabilizes and clean claims behavioral health performance improves.
The Difference Between Billing and Infrastructure
Billing is a task.
Infrastructure is a system that:
- Scrubs claims before submission
- Automates modifier logic
- Detects carve-outs
- Tracks AR aging in real time
- Reduces manual intervention
- Aligns compensation with collected revenue
When claims infrastructure is integrated directly into the EHR and RCM process, revenue leakage drops dramatically.
In our experience, many practices see 10 to 20 percent improvement in insurance revenue simply by eliminating friction.
Not by seeing more patients.
Not by raising rates.
By fixing structure.
Learn more about building infrastructure instead of chasing denials at DENmaar
Final Thought
If you do not measure:
- Clean claim rate
- Rejection percentage
- Denial percentage
- 0 to 30 day AR
- Cost per claim
You are not optimizing revenue.
You are hoping.
Hope is not a revenue strategy.
Frequently Asked Questions
Why do behavioral health practices lose insurance revenue?
Most revenue loss comes from modifier misalignment, Medicaid carve-out errors, eligibility gaps, and fragmented billing infrastructure rather than outright denials.
How much revenue leakage is normal in behavioral health billing?
Many practices unknowingly lose 10 to 20 percent of potential insurance revenue due to preventable structural issues in their EHR and revenue cycle workflow.
Does better billing staff fix revenue leakage?
Not alone. Revenue optimization requires system-level infrastructure that enforces payer rules, authorization logic, and clean claims standards before submission.
How can practices improve Medicaid behavioral health reimbursement?
By integrating eligibility detection, modifier enforcement, authorization tracking, and real time AR monitoring directly into their behavioral health EHR and RCM workflow.
Our Partners
Ready to get started?
Feel free to reach out if you have any questions.