- Respond to callers when staff are busy or unavailable
- Reduce missed opportunities from after-hours and weekend calls
- Provide a more consistent intake and scheduling experience
- Keep communication workflows moving without depending on office hours alone
AI RECEPTIONIST FOR BEHAVIORAL HEALTH
Never Miss a Call, Intake
Opportunity, or Scheduling
Request.
Behavioral health practices lose potential clients every day because calls go
unanswered, staff are busy, or intake requests arrive after hours. DENmaar AI
Receptionist helps practices capture opportunities, improve responsiveness,
and reduce administrative workload.
Immediate Call Response
Behavioral Health Workflows
Integrated Scheduling & Intake
Supported functions include
Built for Behavioral Health Organizations
Unlike generic answering services, DENmaar AI Receptionist is designed specifically for behavioral
health workflows and patient communication needs.
01
New patient intake
Capture initial caller details and support first-contact intake workflows for prospective patients.
02
Appointment Scheduling
Help callers request available appointments and move scheduling requests into the right workflow.
03
Appointment Rescheduling
Support reschedule requests without requiring every call to be handled directly by staff.
04
Frequently Asked Questions
Provide helpful responses to common patient questions about practice operations, locations, or services.
05
Insurance Intake Collection
Collect insurance-related details needed for intake workflows and claims readiness preparation.
06
Message Routing
Route messages and requests to the appropriate team, department, or follow-up queue.
07
After-Hours Call Handling
Respond to callers outside business hours so opportunities are not lost overnight or on weekends.
08
Call Summaries
Provide staff with a concise summary of the call, captured details, and recommended next steps.
09
Provider & Location Routing
Direct patients to the right provider, office, or service line based on their needs and request type.
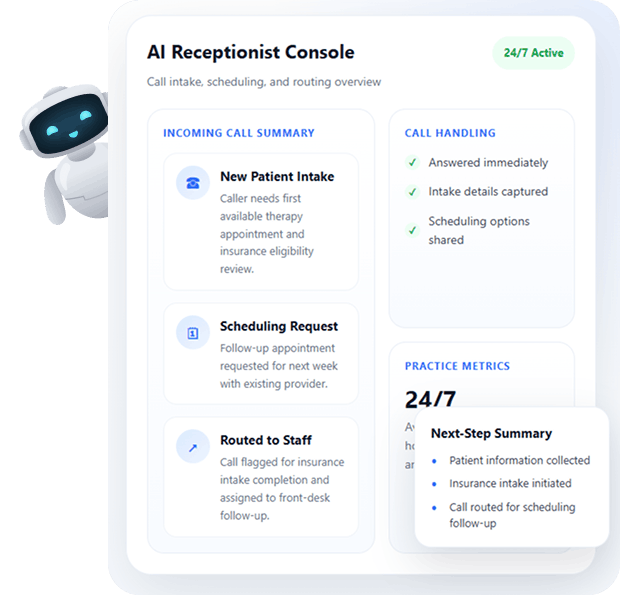
HOW IT WORKS
From Incoming Call to Actionable Next Step
AI Receptionist helps practices respond quickly, collect the right information, and move requests into
scheduling, routing, or follow-up workflows.
Patient calls your practice
AI Receptionist answers immediately
Information is collected and documented
Calls are routed, scheduled, or assigned for follow-up
Staff receive a summary and next steps
AVAILABLE 24/7
Support Call Handling During Business Hours, Evenings, Weekends, and Holidays
The AI Receptionist can answer calls during business hours, evenings, weekends, and holidays, helping ensure every caller receives a professional response and every opportunity has a better chance of being captured.
Coverage Overview
24/7 Support
Business Hours
Support routine call handling, intake questions, and appointment scheduling requests during the workday.
Evenings
Respond to callers outside traditional office hours when prospective patients are often more available.
Weekends
Capture new opportunities and requests that might otherwise wait until Monday or go unanswered.
Holidays
Maintain a professional first response experience even when the office is closed or staff availability is limited.
INTEGRATED WITH THE DENMAAR PLATFORM
Integrated with the DENmaar Platform
Documentation can connect directly to scheduling, treatment plans, assessments, billing workflows,
claims validation, and provider productivity reporting.
Scheduling
Patient Registration
Insurance Intake
DENmaar AI
Receptionist
Receptionist
Documentation Workflows
Billing Operations
Provider Assignments
WHY ORGANIZATIONS CHOOSE DENMAAR
Built to Improve Responsiveness, Reduce Workload, and Support Better Intake Operations
DENmaar AI Receptionist is designed to help behavioral health organizations respond faster, route requests more effectively, and reduce front-desk strain.
- Immediate Call Response
- Reduced Front Desk Workload
- Improved Patient Experience
- Better Intake Consistency
- Behavioral Health Focused Workflows
- Fully Integrated Platform
Request an
AI Receptionist Demo
Experience how DENmaar AI Receptionist can help your organization capture more opportunities,
- Improve responsiveness
- Streamline intake operations.
Request Information
TESTIMONIALS
WHAT OUR CLIENTS SAY
On behalf of everyone at Meadowlark Counseling Services, I want to extend our sincere thanks for the continued improvements you and your team have made to the DENMaar EMR platform. We have been consistently impressed with both the functionality and user-friendly design of the system, which has made a meaningful difference in our day-to-day operations. The intuitive layout and ease of use have allowed our staff to spend less time navigating the system and more time focusing on client care. The regular updates and enhancements reflect your commitment to meeting the evolving needs of providers in the behavioral health and substance use treatment fields. We genuinely look forward to the new features introduced each month and appreciate how responsive the platform has been to the demands of clinical workflows. We have been so pleased with our experience that we’ve taken the opportunity to recommend DENMaar to other professionals in Pennsylvania who are working in the SUD field. Thank you again for your ongoing support and partnership. We are grateful to be working with a company that truly understands the needs of its users. KIndly, Becky Parks on behalf of the entire team at Meadowlark Counseling Services
I referred one of my colleagues Dr Aaron to you he is just starting g his psychology private practice and looking at where to start. I told him hands down you guys are the best billers and have a great EMR and team. He said he reached out just wanted to let you know!
FANTASTIC job keeping things rolling along with any and all of our billing concerns as well as responding to other issues which may well have been out of your wheelhouse. We are VERY grateful to have you and the crew in our corner.
I appreciate you all so much and DENmaar has been such a blessing Donna to our overall operations and success as an expanding company—allowing us to ultimately operate more efficiently, get our claims paid more consistently, ad stay on top of the critical credentialing piece, among other things. Teamwork does in fact, make the dream work. I’ll loop Chris/Isabella in on this message thread too, as I want All of your team to be aware of how much we appreciate our working relationship with DENmaar
Thank you for your diligence!! I appreciate it so much. Thank you Edwina…
Thank you so much Amy! I will be referring to DENmaar as often as I am asked about credentialing services.
Our Latest Blogs
Why Most Behavioral Health Practices Don’t Have a Billing Problem They Have a Claims Communication Problem
Behavioral Health Revenue Cycle Management Requires Better Claims Communication
Behavioral health leaders often assume their revenue challenges come down to billing performance:
“Our billing team isn’t following up enough.”
“We need better denial management.”
“A/R is creeping up—we need more staff.”
Those assumptions feel logical. They’re also usually wrong.
What most practices actually have is a claims communication problem—and until that’s addressed, no amount of staffing, outsourcing, or software switching will consistently fix revenue.
The Illusion of Billing Issues
On the surface, the symptoms point to billing:
- Denials increasing
- Claims sitting unresolved
- Cash flow lagging
So the response becomes:
- Add more follow-up
- Send more emails
- Hire more billers
But step inside the workflow, and a different pattern emerges.
- A denial comes in.
- Someone interprets it.
- A message gets sent.
- The practice is unsure what to do.
- Time passes.
- The claim stalls.
The issue isn’t effort—it’s translation.
The Real Bottleneck: Fragmented Communication
In most systems today, the claims lifecycle looks like this:
- Claim is submitted
- Denial or issue is returned
- A ticket is created
- A team member reviews it
- A message is sent to the practice
- The practice tries to interpret and respond
At each step, context is lost.
A denial code might say one thing—but the actual issue is something else entirely:
- A COB denial that’s really an eligibility sequencing issue
- An authorization denial that should have been caught pre-submission
- A request to “verify insurance” with no explanation of why
So the practice delays, asks questions, or takes the wrong action.
Meanwhile, the claim sits.
Claims don’t stall because they’re complex.
They stall because no one translates them into clear, actionable steps.
The Hidden Cost of Chat and Tickets
Most organizations rely on some combination of:
- Slack or Teams
- Ticketing systems
These tools create the appearance of activity—but they introduce significant inefficiencies:
- Multiple back-and-forth messages per claim
- Repeated explanations of the same issue
- Offshore teams calling payers without full context
- Senior staff acting as translators instead of operators
The result:
- Higher cost per claim
- Slower resolution times
- Increased write-offs
- Frustration across teams
This is where revenue quietly leaks—not from lack of effort, but from lack of structure.
What High-Performance Claims Systems Actually Do
High-performing revenue cycle operations don’t rely on more communication.
They rely on better-structured communication.
That means:
- Every claim has a clear status
- Every issue has a defined root cause
- Every action is explicitly guided
- Every team member sees the same information
Instead of asking:
“What should we do with this claim?”
The system answers:
“Here’s the issue. Here’s why it happened. Here’s the next step.”
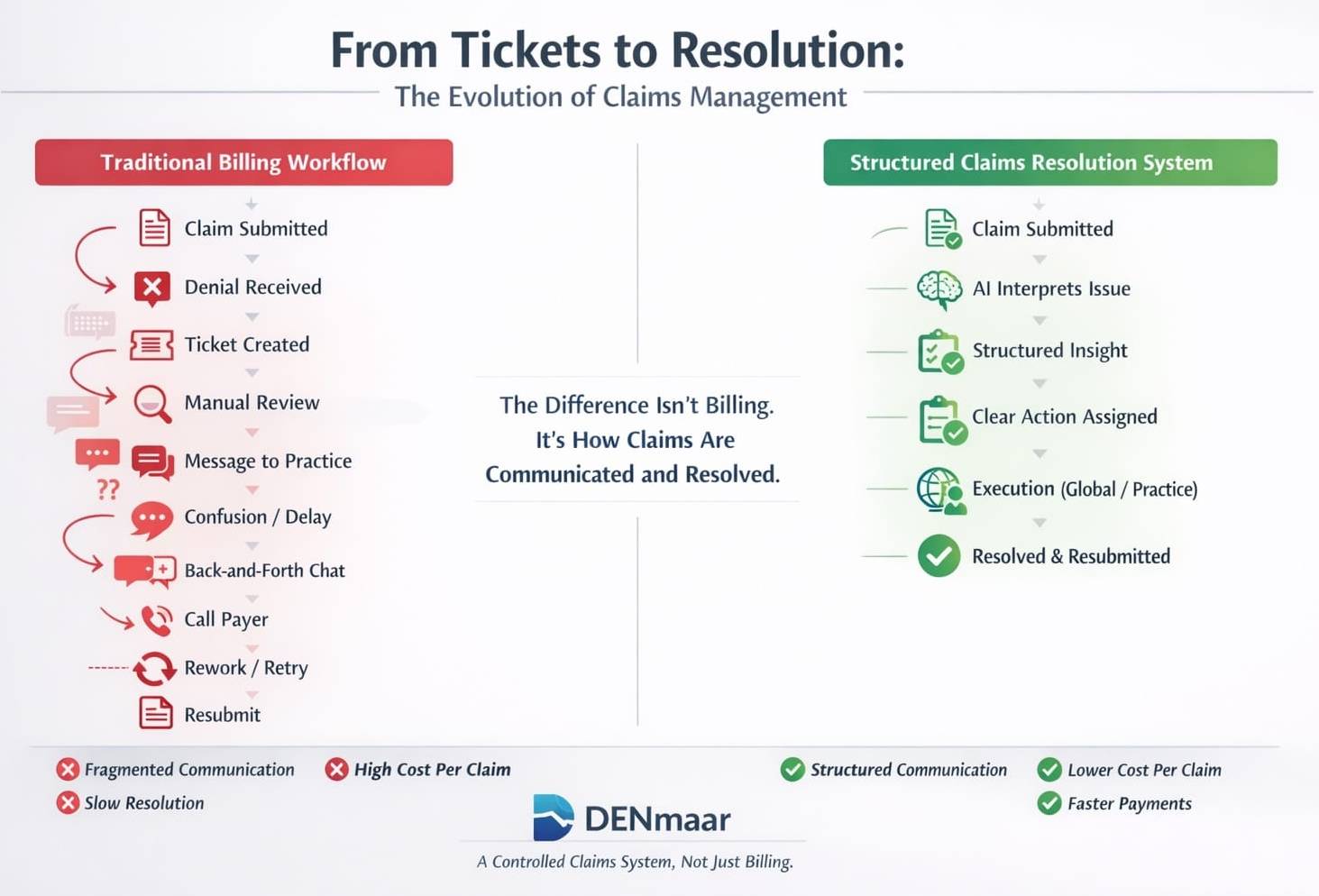
From Tickets to Resolution Systems
Consider the difference:
Traditional Ticket
“Please verify insurance.”
Structured Claims Communication
“Secondary insurance detected. Primary payer likely changed.
Action: Contact patient to confirm active plan and update payer sequence before resubmission.”
One creates confusion.
The other drives resolution.
This shift—from vague tickets to structured, claim-specific guidance—is where performance changes.
Where AI Actually Fits in Behavioral Health Billing
There’s a lot of noise around AI in healthcare right now. Most of it misses the point.
AI is not valuable because it replaces people.
It’s valuable because it standardizes interpretation and accelerates decision-making.
In the claims lifecycle, that means:
- Translating denial codes into real-world causes
- Identifying patterns across payer behavior
- Recommending next steps based on historical outcomes
- Reducing unnecessary payer calls
AI becomes the interpreter and guide, not the operator.
Learn how this works in AI behavioral health billing and clean claims systems.
Why This Breaks at Scale
At low volume, teams can “manage through it.”
At higher volume, the cracks widen:
- 500 claims/month → manageable
- 5,000+ claims/month → breakdown
More claims mean:
- More variability
- More payer nuance
- More communication points
Without a structured system, complexity compounds—and revenue suffers.
What works for a small practice doesn’t scale to a growing group.
The Shift: From Billing to Controlled Claims Systems
The most important shift isn’t hiring more staff or switching vendors.
It’s moving from:
Reactive billing workflows
To:
Controlled claims systems with embedded communication logic
At DENmaar, that’s been the focus:
Not just submitting claims—but controlling the entire lifecycle:
From scheduling
To documentation
To claim generation
To post-submission resolution
With structured communication and embedded intelligence at every step.
This includes:
- Behavioral health EHR software
- Mental health billing services
- Claims hygiene workflows
- AI progress notes for behavioral health
- AI front door patient intake systems
Final Thought
If your team is spending more time explaining claims than resolving them,
you don’t have a staffing issue.
You have a system issue.
And fixing that changes everything:
- Faster payments
- Lower cost per claim
- Less friction across teams
- Stronger, more predictable revenue
That’s where the real leverage is.
Frequently Asked Questions
What is a claims communication problem in behavioral health billing?
A claims communication problem happens when denials, payer issues, and claim tasks are poorly explained across teams, causing delays and lost revenue.
How can behavioral health practices reduce claim delays?
Practices can reduce delays by using structured claims workflows, AI-driven billing intelligence, and integrated revenue cycle management systems.
Does AI replace billing teams?
No. AI improves billing team efficiency by translating denial codes, prioritizing actions, and reducing repetitive manual tasks.
Why do claims problems increase as practices grow?
As claim volume rises, payer complexity, denial volume, and communication bottlenecks increase. Manual systems do not scale efficiently.
What helps improve clean claims rates?
Integrated EHR systems, claims hygiene, payer rule validation, structured documentation, and proactive billing workflows all improve clean claims rates.
Why Behavioral Health Practices Don’t Need an AI Receptionist Anymore
A Better Front Door for Behavioral Health Revenue Cycle Management
Behavioral health organizations have been trying to solve access with the wrong tools.
AI receptionists.
Chatbots.
Call routing systems.
All attempting to replicate a front desk—just with automation.
But here’s the issue:
The problem was never the front desk. It was the model.
The Old Model: Wait for the Patient to Call
Traditional systems assume:
- A patient calls or submits a form
- Staff responds
- Intake is scheduled
- Care begins
AI receptionists simply try to make that process faster.
But they don’t fix the core issue:
Many patients never call in the first place.
The Shift: Patients Enter Care Differently Now
Modern behavioral health demand looks different:
- Patients want privacy
- They explore care before committing
- They engage digitally first
- They decide later whether to identify themselves
This is where platforms like Anonymous Health change the equation.
They don’t wait for the patient to call.
They meet the patient earlier—when they’re still deciding.
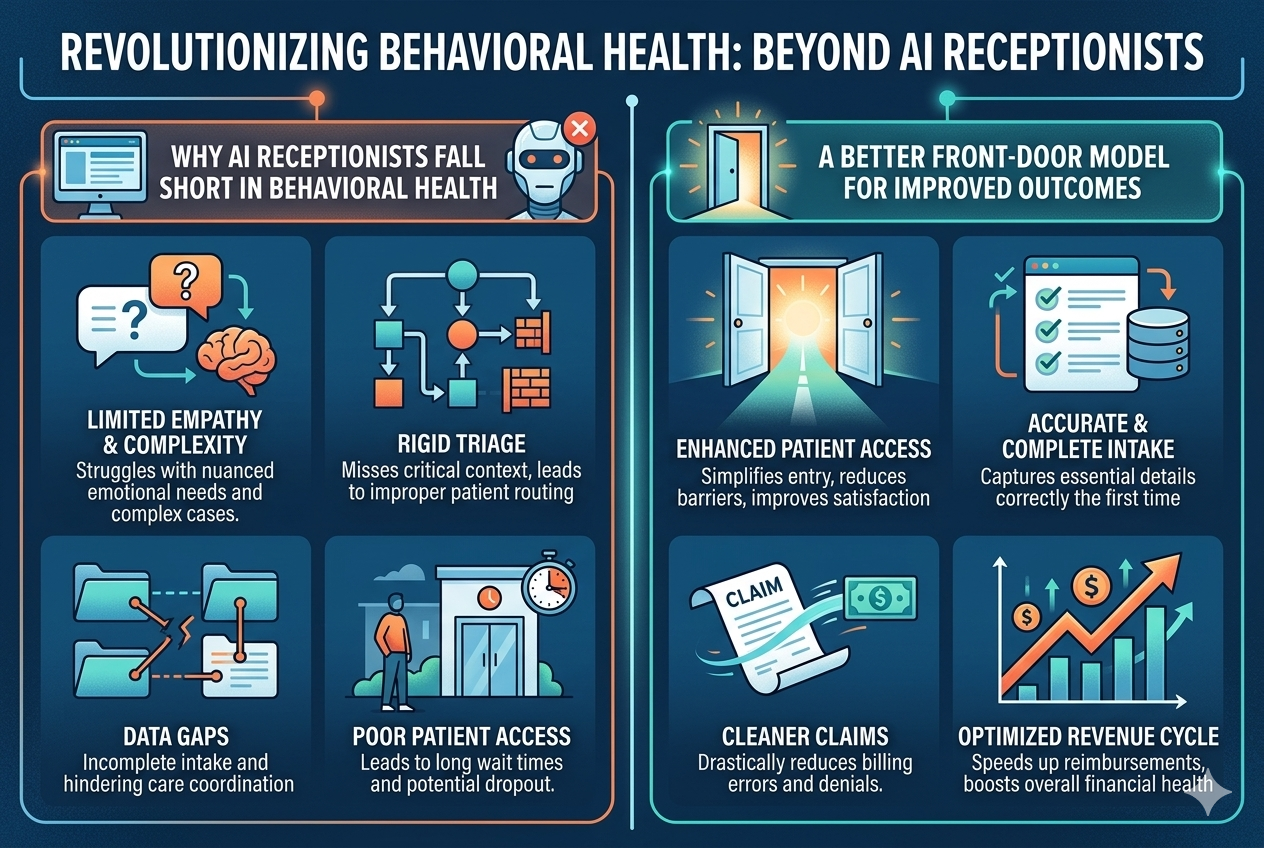
Why AI Receptionists Fall Short in Behavioral Health
AI receptionist platforms still depend on:
- A triggered interaction (call, chat, form)
- A known patient identity
- A defined intake path
They operate inside the old funnel.
So even if optimized, they only improve:
What’s already happening—not what’s missing
The Real Gap: Anonymous Demand to Structured Care
There is a growing layer of demand that never reaches your system:
- Patients browsing silently
- Patients unsure about treatment
- Patients unwilling to identify yet
If your system can’t capture that:
- It never becomes a scheduled visit
- It never becomes a documented session
- It never becomes a claim
A Different Approach: Digital Engagement as the Front Door
At DENmaar, we’ve taken a different approach.
Instead of replacing front desk workflows, we rethink the entry point.
By working with technology partners like Anonymous Health, practices can:
- Capture patient engagement earlier
- Allow anonymous exploration
- Build trust before intake
This is not about automation.
It’s about access transformation.
From Engagement to Revenue: Where Most Systems Break
Most platforms stop at engagement.
They don’t answer:
- How does this patient get scheduled?
- How is care documented?
- How does this become a clean claim?
This is where fragmentation happens.
The DENmaar Model: Close the Loop
DENmaar is designed to connect the entire process through an integrated behavioral health EHR and mental health billing services:
- Digital engagement (including anonymous entry)
- Structured intake → schedulable patient
- AI-supported documentation using AI progress notes
- Claim generation → submission → follow-up powered by AI in behavioral health billing
Every step is tied to revenue.
This model also integrates upstream validation through claims hygiene in behavioral health billing, ensuring clean claims and reducing denials.
Additionally, intake intelligence powered by an AI insurance card reader ensures accurate payer routing and Medicaid billing alignment from the start.
Explore the full system at DENmaar.
What This Replaces
When implemented correctly, this model replaces:
- AI receptionist platforms
- Intake coordination tools
- Disconnected patient engagement systems
Because instead of patching the front desk, you now have:
A system that converts demand directly into billable care
Why This Matters for Growing Practices
For multi-provider behavioral health groups, this shift drives:
- Faster time to first claim
- Higher conversion rates
- Increased provider utilization
- More predictable revenue growth
Who This Is Designed For
This approach is built for practices that are:
- Scaling to multiple providers
- Managing insurance-based revenue
- Looking to grow efficiently—not just add tools
It is not designed for:
- Solo-only providers
- Low-volume, self-pay-only models
Final Thought
AI receptionists try to optimize the front desk.
But behavioral health doesn’t need a better front desk.
It needs a better front door.
And once that door is open, it needs a system that can turn engagement into revenue.
That’s where the real advantage is.
Frequently Asked Questions
Do behavioral health practices need AI receptionists?
Not necessarily. AI receptionists improve response time, but they do not capture anonymous demand or solve upstream revenue cycle issues.
What is the better alternative to AI receptionists?
A digital front-door model that captures early patient engagement and connects it to scheduling, documentation, and billing workflows.
How does this impact behavioral health revenue cycle management?
By connecting engagement to claims, practices improve clean claim rates, reduce denials, and increase revenue without adding more patients.
How does AI help in behavioral health billing?
AI supports claims hygiene, payer routing, documentation accuracy, and pre-submission validation to ensure claims are clean and payable.
Why is early patient engagement important in mental health services?
Because many patients explore care anonymously first. Capturing that stage increases conversion into billable services.
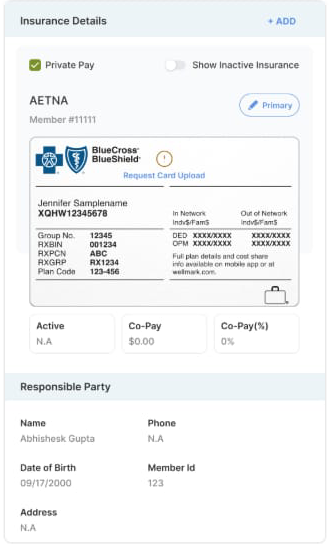
AI Insurance Card Intelligence in Behavioral Health Billing and Revenue Cycle Management
Behavioral health revenue doesn’t break at claim submission. It breaks at intake.
The insurance ID card is the first point of truth in the revenue cycle, yet most systems treat it as a passive data entry step. In reality, this single artifact contains the routing logic that determines whether a claim gets paid or rejected.
For behavioral health practices, especially those operating across therapy, psychiatry, SUD, and higher levels of care, the complexity increases due to mental health carve-outs. These carve-outs separate behavioral health benefits from medical coverage, often assigning them to entirely different payers.
If that distinction is not identified at intake, the downstream impact is immediate: claims are sent to the wrong payer, rejected, corrected, and resubmitted, delaying revenue and increasing administrative burden.
DENmaar approaches this differently by treating the ID card as a structured data source and a decision engine for payer routing.
Practices using modern behavioral health EHR systems and integrated behavioral health billing services increasingly rely on intelligent intake infrastructure to ensure payer accuracy before claims ever reach the clearinghouse.
Learn more about how preventative claims infrastructure for behavioral health billing improves revenue cycle outcomes.
The Core Problem Mental Health Carve Outs Disrupt Standard Billing Logic
Traditional EHR systems capture insurance data in flat fields: payer name, member ID, and group number. This approach assumes that the payer listed on the card is the correct destination for all services.
In behavioral health, that assumption is frequently wrong.
A single insurance card may represent:
- A medical payer such as Blue Cross Blue Shield or Aetna
- A behavioral health carve-out managed by a third party such as Carelon, Optum, or Magellan
- Separate claims addresses or submission pathways depending on service type
Without identifying these distinctions, practices unknowingly submit behavioral health claims to the medical payer. The result is predictable: rejections for incorrect payer routing.
This is not a billing issue. It is an intake intelligence issue.
You can explore how this problem affects claims performance in behavioral health billing revenue cycle failures.
Step 1 Structured Data Extraction Not Basic OCR
Most OCR tools simply convert images into text. That is insufficient for healthcare workflows.
DENmaar’s ID card reader performs structured extraction. It identifies and categorizes specific data elements, including:
- Payer name
- Member ID
- Group number
- RX BIN, PCN, and RX Group
- Plan identifiers
- Claims submission addresses
- Network indicators
Instead of returning raw text, the system maps this information into discrete, usable data fields within the platform.
This creates a normalized dataset that can be used downstream for validation, eligibility checks, and payer routing inside a modern behavioral health EHR platform.
Learn how behavioral health EHR and mental health EHR software integrates these workflows.
Step 2 Carve Out Detection and Interpretation
The critical layer is not extraction. It is an interpretation.
DENmaar analyzes the extracted data for carve-out indicators, including:
- Keywords such as behavioral health, mental health services, or managed by
- Differences in claims addresses that suggest separate submission entities
- Plan structures tied to subcontracted behavioral health networks
- Logo and branding recognition that signal payer relationships
Based on these signals, the system determines whether behavioral health services should be routed to a different payer than the one prominently displayed on the card.
The output is not just a flag, but a routing recommendation embedded into the workflow.
This intelligence contributes to stronger clean claims performance in behavioral health revenue cycle management.
See how this connects to claims hygiene in behavioral health billing.
Step 3 Real Time Payer Routing Within the Workflow
Once a carve-out is detected, that intelligence is applied across the entire revenue cycle.
At the scheduling level, the system associates the correct payer with the appointment based on service type. Therapy, medication management, and higher levels of care can each trigger different routing logic.
At the documentation level, diagnoses and service codes are validated against the expected payer structure to ensure consistency.
AI driven documentation systems also help standardize billing alignment through AI documentation for behavioral health and AI progress notes.
At the daysheet level, where claims are finalized, the system enforces the correct payer destination before submission.
This eliminates one of the most common sources of claim rejection: sending claims to the wrong payer.
Step 4 Alignment with Eligibility and Authorization
Correct payer identification at intake ensures that all subsequent processes are aligned.
Eligibility checks are performed against the appropriate behavioral health payer rather than the medical plan.
Authorization requirements are tracked under the correct entity, preventing mismatches between approved services and submitted claims.
Patient responsibility calculations, including copays and coinsurance, reflect the actual behavioral health benefits rather than generalized medical coverage.
This is particularly important for Medicaid billing behavioral health, psychiatry billing Medicaid, and substance use treatment billing, where carve-outs are common and rules are highly specific.
Organizations managing these workflows often combine EHR infrastructure with behavioral health billing services and mental health billing services.
Step 5 Continuous Learning through Claim Outcomes
DENmaar’s system does not rely solely on static rules. It incorporates feedback from real claim outcomes.
When a claim is rejected due to incorrect payer routing, that data is captured and used to refine future routing decisions.
When a claim is successfully processed and paid, it reinforces the accuracy of the existing logic.
Over time, this creates a continuously improving payer intelligence layer that adapts to real-world variations across plans and regions.
This adaptive intelligence is a core component of RCM for behavioral health and clean claims optimization.
More about the platform approach can be found at:
www.denmaar.com
Financial Impact Why Accurate Payer Routing Matters
Accurate payer routing at intake has a direct and measurable impact on revenue performance.
Practices using an integrated system like DENmaar typically experience:
- A 10 to 20 percent increase in insurance revenue
- Significantly higher clean claim rates
- Reduced administrative time spent on corrections and resubmissions
- Faster reimbursement cycles
These outcomes are not driven by post submission follow up. They are achieved by preventing errors before the claim is ever created.
The Intake to Claim Flywheel
DENmaar’s ID card reader is not an isolated feature. It is the entry point into a larger system designed to optimize claims performance.
The workflow operates as a continuous cycle:
- ID card capture and structured extraction
- Carve out detection and payer interpretation
- Eligibility and authorization alignment
- Scheduler, documentation, and daysheet enforcement
- Clean claim submission
- Feedback loop from claim outcomes
By embedding intelligence at the very beginning of the process, the system ensures that every downstream step operates with accurate, actionable data.
Conclusion
Most systems treat the insurance card as a static input. DENmaar treats it as a dynamic source of payer logic.
By extracting, interpreting, and operationalizing the information contained on the card, the platform ensures that behavioral health claims are routed correctly before submission.
This approach transforms intake from a clerical task into a core component of revenue optimization.
DENmaar does not just read insurance cards. It interprets payer logic in real time, ensuring that every behavioral health claim is sent to the right payer from the start.
Frequently Asked Questions
Why are mental health carve outs important in behavioral health billing?
Mental health carve outs separate behavioral health benefits from medical insurance coverage. If a practice submits claims to the medical payer instead of the behavioral health payer, the claim is often rejected. Correct carve out detection ensures accurate payer routing and higher clean claim rates.
How does AI improve behavioral health revenue cycle management?
AI improves behavioral health revenue cycle management by analyzing payer rules, validating documentation, detecting billing inconsistencies, and ensuring claims are routed to the correct payer before submission.
What is the role of an insurance card reader in behavioral health billing?
An AI insurance card reader extracts structured payer data from insurance cards, detects behavioral health carve outs, and ensures claims are routed correctly. This reduces administrative work and improves Medicaid behavioral health reimbursement.
Why do behavioral health claims get rejected due to payer routing?
Claims are often rejected when the payer responsible for behavioral health services differs from the medical payer on the card. Without carve out detection and payer intelligence, claims may be submitted to the wrong payer.
Our Partners
Ready to get started?
Feel free to reach out if you have any questions.