- Respond to callers when staff are busy or unavailable
- Reduce missed opportunities from after-hours and weekend calls
- Provide a more consistent intake and scheduling experience
- Keep communication workflows moving without depending on office hours alone
AI RECEPTIONIST FOR BEHAVIORAL HEALTH
Never Miss a Call, Intake
Opportunity, or Scheduling
Request.
Behavioral health practices lose potential clients every day because calls go
unanswered, staff are busy, or intake requests arrive after hours. DENmaar AI
Receptionist helps practices capture opportunities, improve responsiveness,
and reduce administrative workload.
Immediate Call Response
Behavioral Health Workflows
Integrated Scheduling & Intake
Supported functions include
Built for Behavioral Health Organizations
Unlike generic answering services, DENmaar AI Receptionist is designed specifically for behavioral
health workflows and patient communication needs.
01
New patient intake
Capture initial caller details and support first-contact intake workflows for prospective patients.
02
Appointment Scheduling
Help callers request available appointments and move scheduling requests into the right workflow.
03
Appointment Rescheduling
Support reschedule requests without requiring every call to be handled directly by staff.
04
Frequently Asked Questions
Provide helpful responses to common patient questions about practice operations, locations, or services.
05
Insurance Intake Collection
Collect insurance-related details needed for intake workflows and claims readiness preparation.
06
Message Routing
Route messages and requests to the appropriate team, department, or follow-up queue.
07
After-Hours Call Handling
Respond to callers outside business hours so opportunities are not lost overnight or on weekends.
08
Call Summaries
Provide staff with a concise summary of the call, captured details, and recommended next steps.
09
Provider & Location Routing
Direct patients to the right provider, office, or service line based on their needs and request type.
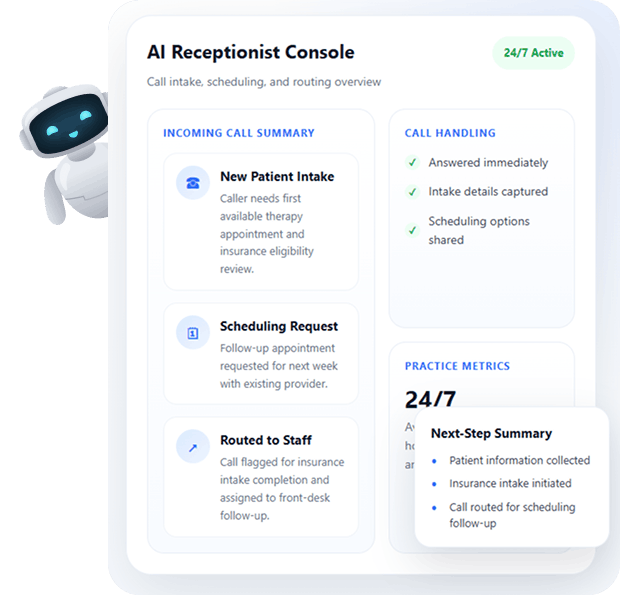
HOW IT WORKS
From Incoming Call to Actionable Next Step
AI Receptionist helps practices respond quickly, collect the right information, and move requests into
scheduling, routing, or follow-up workflows.
Patient calls your practice
AI Receptionist answers immediately
Information is collected and documented
Calls are routed, scheduled, or assigned for follow-up
Staff receive a summary and next steps
AVAILABLE 24/7
Support Call Handling During Business Hours, Evenings, Weekends, and Holidays
The AI Receptionist can answer calls during business hours, evenings, weekends, and holidays, helping ensure every caller receives a professional response and every opportunity has a better chance of being captured.
Coverage Overview
24/7 Support
Business Hours
Support routine call handling, intake questions, and appointment scheduling requests during the workday.
Evenings
Respond to callers outside traditional office hours when prospective patients are often more available.
Weekends
Capture new opportunities and requests that might otherwise wait until Monday or go unanswered.
Holidays
Maintain a professional first response experience even when the office is closed or staff availability is limited.
INTEGRATED WITH THE DENMAAR PLATFORM
Integrated with the DENmaar Platform
Documentation can connect directly to scheduling, treatment plans, assessments, billing workflows,
claims validation, and provider productivity reporting.
Scheduling
Patient Registration
Insurance Intake
DENmaar AI
Receptionist
Receptionist
Documentation Workflows
Billing Operations
Provider Assignments
WHY ORGANIZATIONS CHOOSE DENMAAR
Built to Improve Responsiveness, Reduce Workload, and Support Better Intake Operations
DENmaar AI Receptionist is designed to help behavioral health organizations respond faster, route requests more effectively, and reduce front-desk strain.
- Immediate Call Response
- Reduced Front Desk Workload
- Improved Patient Experience
- Better Intake Consistency
- Behavioral Health Focused Workflows
- Fully Integrated Platform
Request an
AI Receptionist Demo
Experience how DENmaar AI Receptionist can help your organization capture more opportunities,
- Improve responsiveness
- Streamline intake operations.
Request Information
TESTIMONIALS
WHAT OUR CLIENTS SAY
On behalf of everyone at Meadowlark Counseling Services, I want to extend our sincere thanks for the continued improvements you and your team have made to the DENMaar EMR platform. We have been consistently impressed with both the functionality and user-friendly design of the system, which has made a meaningful difference in our day-to-day operations. The intuitive layout and ease of use have allowed our staff to spend less time navigating the system and more time focusing on client care. The regular updates and enhancements reflect your commitment to meeting the evolving needs of providers in the behavioral health and substance use treatment fields. We genuinely look forward to the new features introduced each month and appreciate how responsive the platform has been to the demands of clinical workflows. We have been so pleased with our experience that we’ve taken the opportunity to recommend DENMaar to other professionals in Pennsylvania who are working in the SUD field. Thank you again for your ongoing support and partnership. We are grateful to be working with a company that truly understands the needs of its users. KIndly, Becky Parks on behalf of the entire team at Meadowlark Counseling Services
I referred one of my colleagues Dr Aaron to you he is just starting g his psychology private practice and looking at where to start. I told him hands down you guys are the best billers and have a great EMR and team. He said he reached out just wanted to let you know!
FANTASTIC job keeping things rolling along with any and all of our billing concerns as well as responding to other issues which may well have been out of your wheelhouse. We are VERY grateful to have you and the crew in our corner.
I appreciate you all so much and DENmaar has been such a blessing Donna to our overall operations and success as an expanding company—allowing us to ultimately operate more efficiently, get our claims paid more consistently, ad stay on top of the critical credentialing piece, among other things. Teamwork does in fact, make the dream work. I’ll loop Chris/Isabella in on this message thread too, as I want All of your team to be aware of how much we appreciate our working relationship with DENmaar
Thank you for your diligence!! I appreciate it so much. Thank you Edwina…
Thank you so much Amy! I will be referring to DENmaar as often as I am asked about credentialing services.
Our Latest Blogs

Why We Replaced Free Trials with a Claims Submission Pilot Program
In behavioral healthcare, selecting an EHR and billing partner is one of the most important operational decisions a practice will make.
Unfortunately, many software companies still rely on the traditional “free trial” model. Practices receive access to a system, click around for a few days, and then are expected to make a long-term decision based on limited experience.
We believe there is a better way.
At DENmaar, we replaced traditional free trials with a structured Claims Submission Pilot Program.
Why Free Trials Often Fail
The reality is that most behavioral health practices do not determine success based on whether a scheduler looks attractive or a progress note can be completed.
Success is determined by questions such as:
- Are claims being paid?
- Are providers completing documentation on time?
- Is eligibility being verified correctly?
- Are authorizations being managed effectively?
- Is insurance revenue increasing?
- Is administrative burden decreasing?
A traditional free trial rarely answers these questions.
The Purpose of a Pilot Program
A pilot allows both organizations to determine whether there is a true operational fit.
Instead of evaluating screenshots and demonstrations, practices can evaluate real workflows using real providers, real patients, and real claims.
During a DENmaar pilot, organizations gain access to:
- Behavioral health EHR workflows
- Scheduling and appointment management
- Eligibility and benefits verification
- AI-powered clinical documentation tools
- Claims submission and behavioral health revenue cycle management
- Credentialing support
- Weekly implementation and optimization meetings
The objective is simple: validate results.
Measuring Success
By the conclusion of a pilot, leadership should have clear answers to several critical questions.
Clinical Operations
- Are providers documenting efficiently?
- Are notes being completed on time?
- Is clinical compliance improving?
Revenue Cycle Performance
- Are claims submitting cleanly?
- Are rejection rates decreasing?
- Are billing workflows becoming more efficient?
Organizational Fit
- Does the platform support the organization’s long-term goals?
- Can the system scale as additional providers are added?
- Does the support model align with leadership expectations?
Not Every Organization Is a Fit
One of the most important aspects of our pilot program is qualification.
DENmaar is designed primarily for organizations that are building or operating multi-provider behavioral health practices.
Organizations that are focused on growth, operational discipline, and insurance-based care typically receive the most value from our platform.
For that reason, we do not believe every inquiry should automatically receive a pilot.
We would rather identify strong mutual fit upfront than create unrealistic expectations for either organization.
Why We Built DENmaar
DENmaar was created around a simple belief:
Behavioral health organizations should not have to choose between great software and great billing support.
Most organizations purchase software from one company, credentialing from another, billing services from a third, and then spend countless hours coordinating between them.
We chose a different approach.
DENmaar combines behavioral health technology, revenue cycle management, credentialing, eligibility verification, and operational support into a single platform designed to help organizations improve efficiency and increase insurance revenue.
Organizations looking to strengthen their behavioral health insurance billing infrastructure can learn more about the 3 pillars of successful behavioral health insurance billing.
For practices serving Medicaid populations, understanding Medicaid billing behavioral health requirements is essential for reducing denials and improving reimbursement outcomes.
Many organizations also struggle when determining payer hierarchy and coordination of benefits. Understanding when Medicaid is not primary in behavioral health billing can prevent costly claim delays and rework.
Because at the end of the day, successful behavioral health organizations need more than software.
They need systems that produce measurable results.
Interested in a Pilot?
If your organization is a multi-provider behavioral health practice seeking to improve operations, strengthen revenue cycle performance, and scale efficiently, a DENmaar Claims Submission Pilot may be the right next step.
The goal is not to evaluate software.
The goal is to validate results.
Frequently Asked Questions
What is a Claims Submission Pilot Program?
A Claims Submission Pilot Program allows behavioral health organizations to test real-world workflows, claims submission processes, eligibility verification, provider credentialing, and revenue cycle management before committing to a long-term platform.
How is a pilot different from a free trial?
A free trial typically focuses on software access. A pilot focuses on measurable operational outcomes, including clean claims rates, documentation compliance, reimbursement performance, and administrative efficiency.
Who benefits most from a DENmaar pilot?
Multi-provider behavioral health organizations, psychiatry groups, substance use treatment programs, and insurance-based practices typically receive the greatest value from a structured pilot program.
Does the pilot include Medicaid billing workflows?
Yes. The pilot is designed to support complex behavioral health reimbursement scenarios, including Medicaid billing, eligibility verification, authorization management, provider credentialing, and clean claims submission.
Why is revenue cycle management important when selecting a behavioral health EHR?
A behavioral health EHR should support documentation, scheduling, eligibility verification, claims management, and reimbursement workflows. Without integrated revenue cycle management, practices often experience denials, delayed payments, and lost revenue.
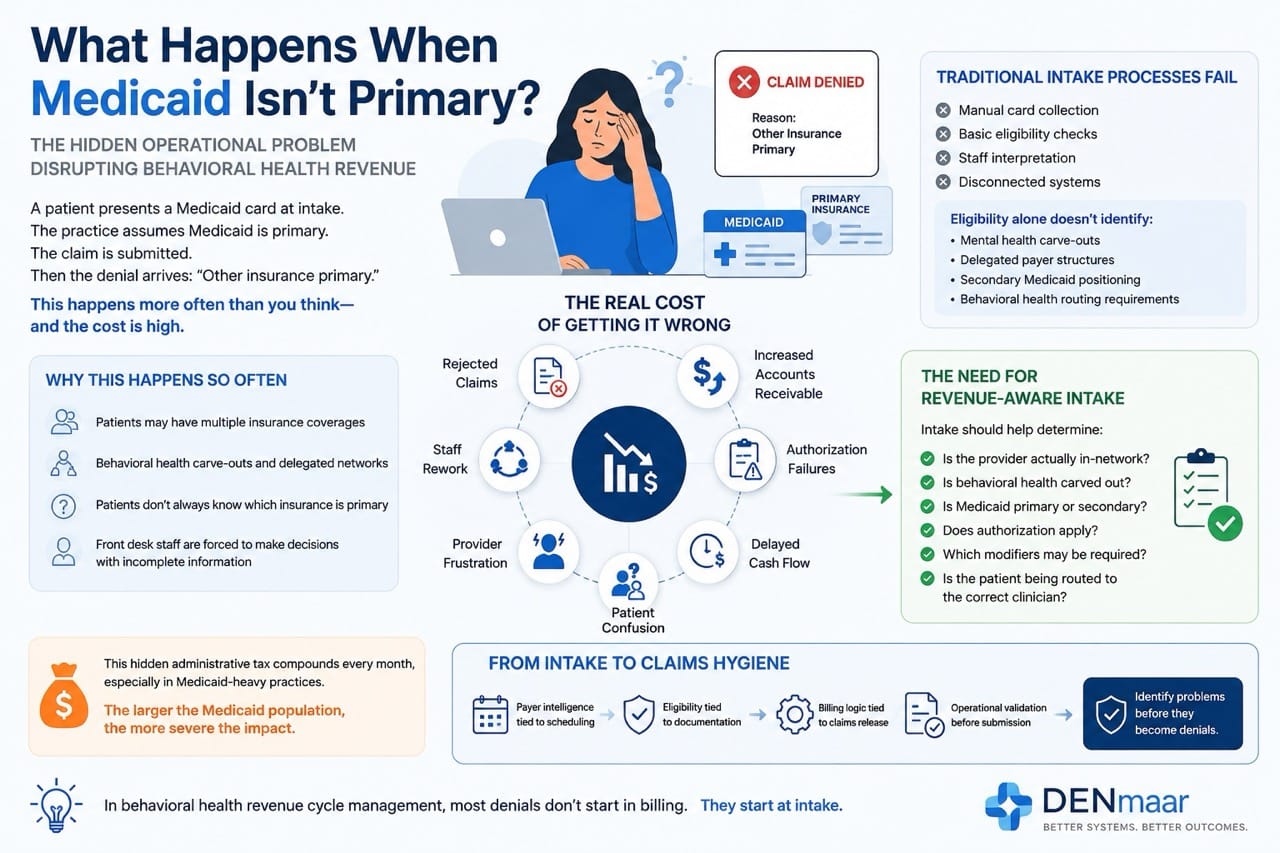
What Happens When Medicaid Isn’t Primary?
The Hidden Operational Problem Disrupting Behavioral Health Revenue
In behavioral health, one of the most common causes of claim delays, denials, and administrative confusion starts before the patient is even seen.
A patient presents a Medicaid card at intake.
The practice assumes Medicaid is primary.
The claim is submitted.
Then the denial arrives:
“Other insurance primary.”
This happens constantly across behavioral health organizations, especially in multidisciplinary practices serving Medicaid populations.
And in many cases, the issue is not billing staff performance.
It is a system failure.
Why This Happens So Often
Behavioral health insurance workflows are uniquely complicated because Medicaid is frequently not the true primary payer.
Patients may have:
- Employer sponsored commercial insurance
- Marketplace plans
- Medicare Advantage
- Managed Medicaid organizations (MCOs)
- Behavioral health carve outs
- Secondary Medicaid eligibility
- County or state funded programs
The challenge is that patients often do not understand:
- Which insurance is primary
- Whether behavioral health is carved out
- Whether a payer delegated services elsewhere
- Whether the provider is actually in network
Front desk teams are then forced to make operational decisions using incomplete information.
The Real Cost of Getting This Wrong
When payer hierarchy is incorrect, the impact spreads across the organization.
Common outcomes include:
- Rejected claims
- Timely filing delays
- Staff rework
- Increased accounts receivable
- Authorization failures
- Provider frustration
- Delayed cash flow
- Patient confusion
In many practices, this creates a hidden administrative tax that compounds every month.
The larger the Medicaid population, the more severe the issue becomes.
Behavioral Health Is Different
Most general healthcare systems were not designed around behavioral health payer complexity.
Behavioral health frequently involves:
- Carve out payers
- Delegated networks
- County plans
- Separate behavioral health administrators
- Program based billing
- Telehealth modifiers
- Medicaid specific requirements
- Mixed institutional and professional claims
A patient’s medical insurance card alone often does not tell the full story.
That means practices need operational workflows capable of identifying:
- The true payer pathway
- Behavioral health delegation
- Provider participation status
- Authorization requirements
- Coordination of benefits
Before claims are released.
Why Traditional Intake Processes Fail
Most intake workflows still rely on:
- Manual card collection
- Basic eligibility checks
- Staff interpretation
- Disconnected systems
But eligibility alone does not always identify:
- Mental health carve outs
- Delegated payer structures
- Secondary Medicaid positioning
- Behavioral health routing requirements
This leaves staff trying to solve payer architecture manually.
At scale, that becomes unsustainable.
The Need for Revenue Aware Intake
The future of behavioral health intake is not simply online scheduling.
It is:
Revenue aware operational intake.
That means intake systems should help determine:
- Is the provider actually in the network?
- Is behavioral health carved out?
- Is Medicaid primary or secondary?
- Does authorization apply?
- Which modifiers may be required?
- Is the patient being routed to the correct clinician?
This is where behavioral health systems must evolve beyond generic scheduling tools.
From Intake to Claims Hygiene
At DENmaar, we believe intake should connect directly into operational claims workflows.
That means:
- Payer intelligence tied to scheduling
- Eligibility tied to documentation
- Billing logic tied to claims release
- Operational validation before submission
We call this approach:
The objective is simple:
Identify problems before they become denials.
Because in behavioral health revenue cycle management, most denials do not start in billing.
They start at intake.
Organizations looking to strengthen payer validation and clean claims performance can also benefit from a behavioral health EHR platform that connects intake, documentation, eligibility, and claims workflows into a unified operational system.
Integrated AI documentation for behavioral health and AI driven claims intelligence further support clean claims behavioral health outcomes and Medicaid behavioral health reimbursement accuracy.
Final Thoughts
Behavioral health organizations do not need more disconnected software.
They need systems designed around the operational realities of behavioral healthcare reimbursement.
As Medicaid complexity continues to grow, practices that modernize intake and payer validation workflows will gain a major operational advantage:
- Fewer denials
- Faster payments
- Lower administrative burden
- Improved patient access
- Stronger financial stability
The future of behavioral health infrastructure will belong to organizations that understand one thing clearly:
Revenue integrity begins before the first appointment is scheduled.
Frequently Asked Questions
Why is Medicaid not always the primary payer?
Many patients have multiple insurance plans. Commercial insurance, Medicare, or managed care plans may be primary while Medicaid serves as a secondary payer. Proper coordination of benefits is essential to prevent claim denials.
What are behavioral health carve outs?
Behavioral health carve outs occur when mental health or substance use treatment services are administered by a separate payer, network, or organization rather than the patient’s primary medical insurer.
How do payer hierarchy errors affect behavioral health billing?
Incorrect payer hierarchy can result in rejected claims, delayed reimbursements, authorization issues, increased accounts receivable, and significant administrative rework.
What is revenue aware intake?
Revenue aware intake is an operational approach that validates payer information, behavioral health carve outs, provider participation status, authorization requirements, and billing pathways before care is delivered.
How does Claims Hygiene improve reimbursement outcomes?
Claims Hygiene identifies eligibility, documentation, payer routing, and billing issues before claims are submitted. This helps reduce denials, improve clean claim rates, and strengthen Medicaid behavioral health reimbursement performance.
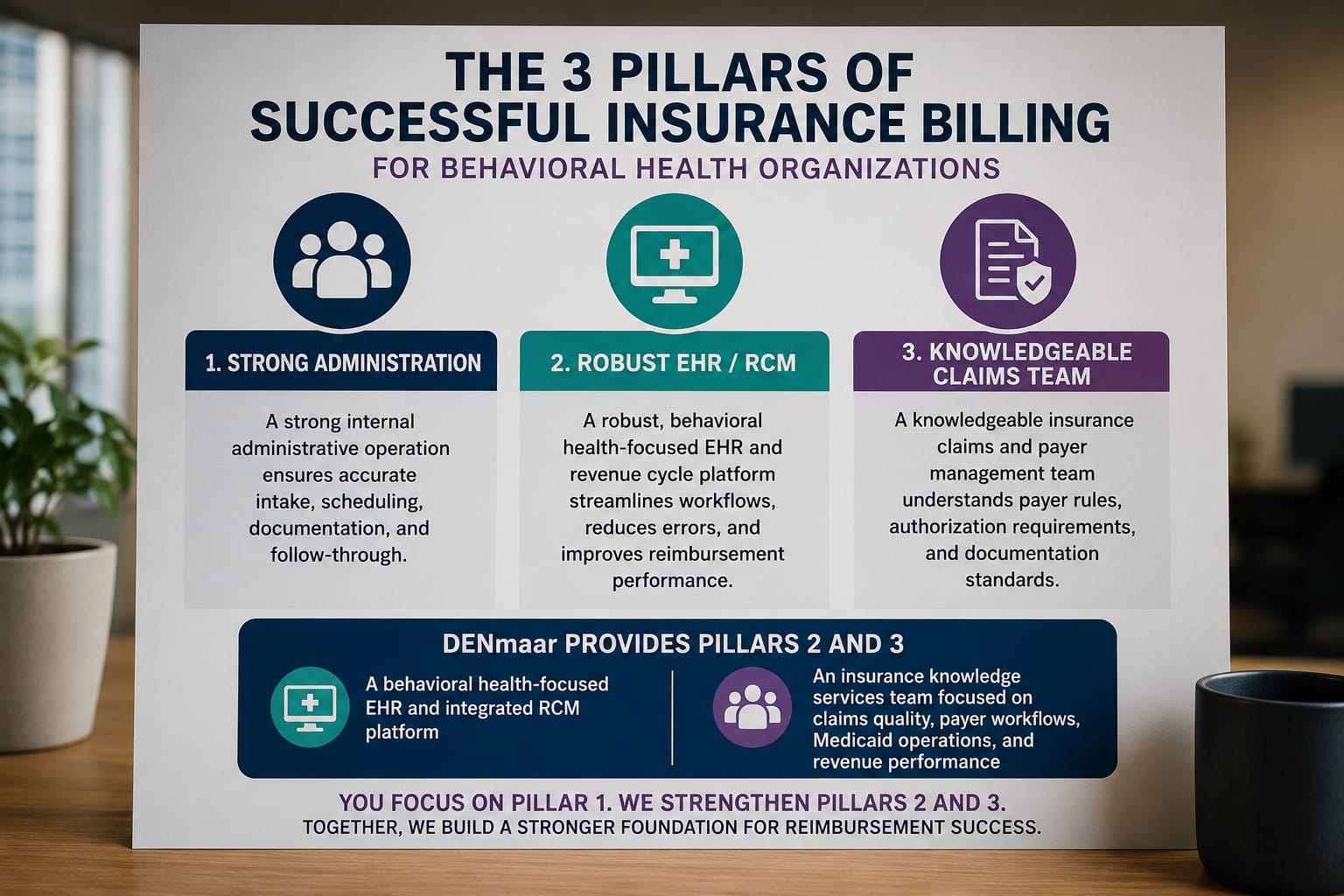
The 3 Pillars of Successful Behavioral Health Insurance Billing
The 3 pillars of successful behavioral health insurance billing:
- A strong internal administrative operation
- A robust behavioral health focused EHR and revenue cycle platform
- A knowledgeable insurance claims and payer management team
Most organizations struggle because one or more of these pillars are weak or disconnected.
DENmaar was built specifically to strengthen pillars 2 and 3.
We provide:
- A behavioral health focused EHR and integrated RCM for behavioral health platform designed around real payer complexity
- An insurance knowledge services team focused on claims quality, payer workflows, Medicaid operations, and revenue performance
This allows practices to focus on building strong clinical and administrative operations while DENmaar helps support the infrastructure behind successful insurance reimbursement.
Organizations looking to improve clean claims behavioral health performance and reduce denials can also explore our approach to claims hygiene for behavioral health billing, behavioral health billing services, and AI powered behavioral health revenue cycle management.
Integrated AI progress notes for behavioral health also help strengthen documentation quality, Medicaid behavioral health reimbursement workflows, and overall revenue cycle accuracy.
Frequently Asked Questions
What are the 3 pillars of successful behavioral health insurance billing?
The 3 pillars are strong administrative operations, a behavioral health EHR and revenue cycle platform, and an experienced insurance claims and payer management team.
Why is a behavioral health focused EHR important?
A behavioral health EHR helps organizations manage Medicaid billing behavioral health workflows, claims hygiene, documentation accuracy, and integrated revenue cycle management more effectively.
How does DENmaar support behavioral health revenue cycle management?
DENmaar combines a behavioral health focused EHR, integrated RCM for behavioral health, payer workflow expertise, and claims management infrastructure to improve reimbursement performance and reduce operational friction.
Our Partners
Ready to get started?
Feel free to reach out if you have any questions.