The Hidden Operational Problem Disrupting Behavioral Health Revenue
In behavioral health, one of the most common causes of claim delays, denials, and administrative confusion starts before the patient is even seen.
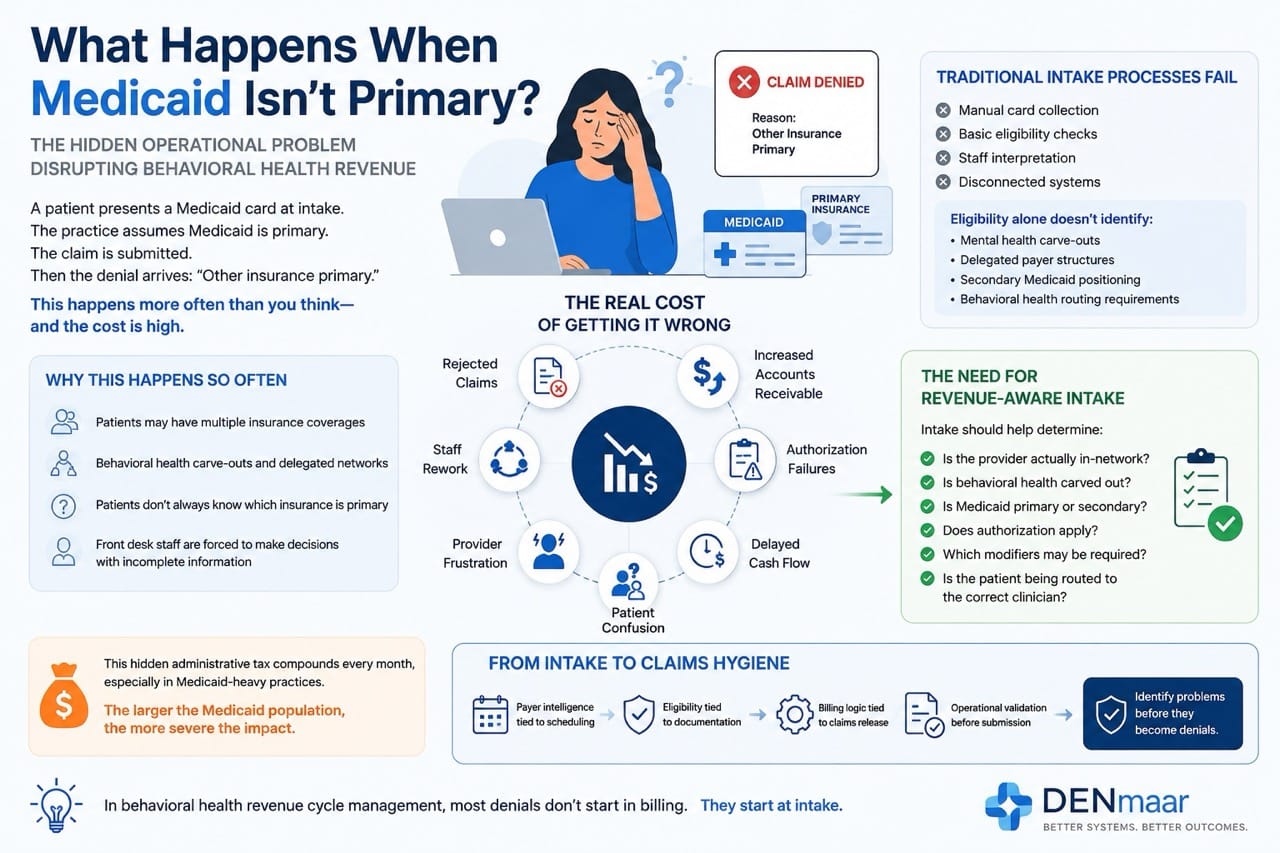
A patient presents a Medicaid card at intake.
The practice assumes Medicaid is primary.
The claim is submitted.
Then the denial arrives:
“Other insurance primary.”
This happens constantly across behavioral health organizations, especially in multidisciplinary practices serving Medicaid populations.
And in many cases, the issue is not billing staff performance.
It is a system failure.
Why This Happens So Often
Behavioral health insurance workflows are uniquely complicated because Medicaid is frequently not the true primary payer.
Patients may have:
- Employer sponsored commercial insurance
- Marketplace plans
- Medicare Advantage
- Managed Medicaid organizations (MCOs)
- Behavioral health carve outs
- Secondary Medicaid eligibility
- County or state funded programs
The challenge is that patients often do not understand:
- Which insurance is primary
- Whether behavioral health is carved out
- Whether a payer delegated services elsewhere
- Whether the provider is actually in network
Front desk teams are then forced to make operational decisions using incomplete information.
The Real Cost of Getting This Wrong
When payer hierarchy is incorrect, the impact spreads across the organization.
Common outcomes include:
- Rejected claims
- Timely filing delays
- Staff rework
- Increased accounts receivable
- Authorization failures
- Provider frustration
- Delayed cash flow
- Patient confusion
In many practices, this creates a hidden administrative tax that compounds every month.
The larger the Medicaid population, the more severe the issue becomes.
Behavioral Health Is Different
Most general healthcare systems were not designed around behavioral health payer complexity.
Behavioral health frequently involves:
- Carve out payers
- Delegated networks
- County plans
- Separate behavioral health administrators
- Program based billing
- Telehealth modifiers
- Medicaid specific requirements
- Mixed institutional and professional claims
A patient’s medical insurance card alone often does not tell the full story.
That means practices need operational workflows capable of identifying:
- The true payer pathway
- Behavioral health delegation
- Provider participation status
- Authorization requirements
- Coordination of benefits
Before claims are released.
Why Traditional Intake Processes Fail
Most intake workflows still rely on:
- Manual card collection
- Basic eligibility checks
- Staff interpretation
- Disconnected systems
But eligibility alone does not always identify:
- Mental health carve outs
- Delegated payer structures
- Secondary Medicaid positioning
- Behavioral health routing requirements
This leaves staff trying to solve payer architecture manually.
At scale, that becomes unsustainable.
The Need for Revenue Aware Intake
The future of behavioral health intake is not simply online scheduling.
It is:
Revenue aware operational intake.
That means intake systems should help determine:
- Is the provider actually in the network?
- Is behavioral health carved out?
- Is Medicaid primary or secondary?
- Does authorization apply?
- Which modifiers may be required?
- Is the patient being routed to the correct clinician?
This is where behavioral health systems must evolve beyond generic scheduling tools.
From Intake to Claims Hygiene
At DENmaar, we believe intake should connect directly into operational claims workflows.
That means:
- Payer intelligence tied to scheduling
- Eligibility tied to documentation
- Billing logic tied to claims release
- Operational validation before submission
We call this approach:
The objective is simple:
Identify problems before they become denials.
Because in behavioral health revenue cycle management, most denials do not start in billing.
They start at intake.
Organizations looking to strengthen payer validation and clean claims performance can also benefit from a behavioral health EHR platform that connects intake, documentation, eligibility, and claims workflows into a unified operational system.
Integrated AI documentation for behavioral health and AI driven claims intelligence further support clean claims behavioral health outcomes and Medicaid behavioral health reimbursement accuracy.
Final Thoughts
Behavioral health organizations do not need more disconnected software.
They need systems designed around the operational realities of behavioral healthcare reimbursement.
As Medicaid complexity continues to grow, practices that modernize intake and payer validation workflows will gain a major operational advantage:
- Fewer denials
- Faster payments
- Lower administrative burden
- Improved patient access
- Stronger financial stability
The future of behavioral health infrastructure will belong to organizations that understand one thing clearly:
Revenue integrity begins before the first appointment is scheduled.