- Therapy and medication management
- IOP, PHP, and SUD treatment programs
- Case management, community support, and residential services
DENmaar Revenue Cycle Intelligence
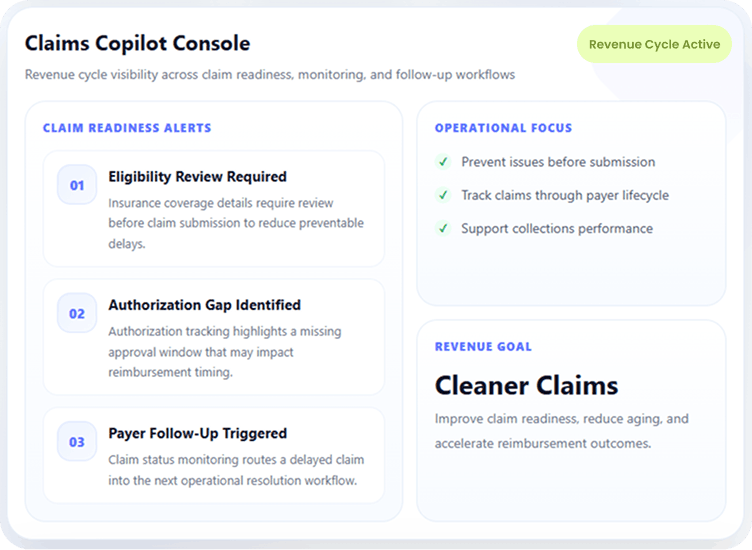
Claims Copilot ™
Stop Chasing Claims.
Start Preventing Problems.
Claims Copilot is DENmaar’s behavioral health revenue cycle solution
designed to help practices prevent claim issues before submission, reduce
aging, accelerate reimbursement, and improve operational performance.
Pre-Submission Claim Readiness
Payer Lifecycle Monitoring
Aging & Collections Visibility
Pre-Submission Readiness
Catch eligibility, authorization, payer, and documentation issues before claims go out.
Lifecycle Claim Monitoring
Track claims after submission with rejection management, status visibility, and aging oversight.
Operational Performance
Support clean claim performance, reduce aged claims, and improve collections visibility.
Behavioral Health Focused
Designed for therapy, medication management, SUD, IOP/PHP, community support, and more.
Built for Behavioral Health
Designed for Behavioral Health
Revenue Cycle Workflows
Whether your organization provides therapy, medication management, IOP,
PHP, SUD treatment, case management, community support, or residential
services, Claims Copilot is built around the operational and reimbursement
realities of behavioral health.
Behavioral health support areas
Claims Copilot is positioned to support behavioral health organizations that need stronger claim readiness, reimbursement visibility, and operational follow-up across complex service lines.
Prevent Problems Before Claims Are Submitted
Address Revenue Cycle Breakdowns
Before They Turn Into Denials or Delays
Most claim problems begin long before a claim is submitted. Claims Copilot helps practices identify and
resolve those issues earlier so reimbursement performance is not undermined later.
Verify Insurance Eligibility
Confirm insurance coverage details early to reduce preventable reimbursement delays and billing confusion.
Review Insurance Information & ID Cards
Validate insurance information and supporting details so claims are built on more accurate payer data.
Track Authorizations
Monitor authorization requirements and approval status to reduce avoidable denials tied to missing coverage approvals.
Monitor Provider Credentialing Requirements
Support awareness of credentialing-related payer requirements that can affect billing and reimbursement workflows.
Identify Claim Issues Before Submission
Catch missing information, workflow gaps, and other claim barriers before the claim enters the payer lifecycle.
Improve Documentation-to-Billing Alignment
Route messages and requests to the appropriate team, department, or follow-up queue.
How Claims Copilot Works
A continuous workflow built to
support prevention, monitoring, and resolution.
Claims Copilot doesn’t stop at submission. It supports the operational work needed before the claim goes out, then continues
tracking activity through the payer lifecycle to help teams reduce delays, aging, and reimbursement bottlenecks.
1
Review claim readiness before submission
Insurance, eligibility, authorization, and workflow details are reviewed to identify claim risks before they become downstream reimbursement problems.
2
Submit claims and monitor payer activity
Once claims are submitted, Claims Copilot supports visibility into rejections, claim status, aging, and other signals that indicate a claim may require action.
3
Route follow-up through the right workflow
Operational tasks can be prioritized based on the issue—whether the next step involves internal follow-up, claim correction, payer research, or payment posting support.
From prevention to reimbursement performance.
Claims Copilot is designed to help organizations manage the full payer journey—not just claim submission. The result is a more proactive revenue cycle process with clearer visibility and fewer avoidable surprises.
Before submission:
improve readiness across insurance, authorizations, and documentation alignment
After submission:
monitor claim status, rejections, denial patterns, and aging across the payer lifecycle.
Operationally:
help teams reduce aging, recover delayed payments, and improve turnaround performance.
Monitor Claims Through the Entire Payer Lifecycle
Submitting claims is only the beginning.
Claims Copilot continuously tracks claim progress and supports the workflows needed to identify
reimbursement issues, respond to payer friction, and keep claims moving toward payment.
Claim Submission & Rejection Visibility
Support clean electronic claim submission while maintaining visibility into rejections and claim issues that need attention after submission.
- Electronic claim submission
- Rejection management support
- Visibility into claim readiness breakdowns
Status Monitoring & Aging Analysis
Track claims after submission to identify delays, payer inactivity, unresolved statuses, and aging trends that can impact collections.
- Claim status monitoring
- Aging analysis and prioritization
- Operational follow-up workflow visibility
Denials, Follow-Up & Payment Support
Improve follow-through on denied or delayed claims by supporting structured next steps across payer follow-up, resolution activity, and payment posting workflows.
- Denial tracking
- Follow-up workflow support
- Payment posting support
Reduce Aging and Improve Collections
Give your organization earlier visibility, better follow-through, and fewer preventable delays.
Many behavioral health organizations struggle with growing accounts receivable because claim issues are discovered too late. Claims Copilot helps teams stay ahead of the work required to keep reimbursement moving.
Reduce aged claims
improve readiness across insurance, authorizations, and documentation alignment.
Recover delayed payments
Identify unresolved payer issues sooner and reduce the amount of time claims spend waiting without meaningful action.
Improve turnaround and clean claim performance
Support stronger revenue cycle performance by reducing preventable breakdowns before and after submission.
A Partnership Approach
Successful revenue cycle management requires operational collaboration.
Many behavioral health organizations struggle with growing accounts receivable because claim issues are discovered too late. Claims Copilot helps teams stay ahead of the work required to keep reimbursement moving.
Before submission:
improve readiness across insurance, authorizations, and documentation alignment.
After submission:
monitor claim status, rejections, denial patterns, and aging across the payer lifecycle.
Operationally:
help teams reduce aging, recover delayed payments, and improve turnaround performance.
Included With DENmaar
Claims Copilot is part of the DENmaar
Behavioral Productivity Platform.
When DENmaar manages your insurance billing, your organization also gains access to the broader operational and clinical
platform that supports scheduling, documentation, reporting, and patient management workflows.
Behavioral Health EHR
Clinical and operational workflows designed around behavioral health documentation and care delivery.
Scheduling
Integrated scheduling workflows to support patient flow, operational visibility, and billing readiness.
Documentation Tools
Clinical notes, treatment plans, and documentation workflows that support stronger operational alignment.
AI-Assisted Notes
Support documentation efficiency while maintaining professional review and oversight workflows.
Treatment Plans
Behavioral health planning tools that connect care planning with documentation and operational workflows.
Clinical Workflows
Support multidisciplinary behavioral health processes with connected operational and clinical workflows.
Reporting
Visibility into productivity, claim performance, and operational trends across the platform.
Patient Management Tools
Connected workflows for patient registration, intake coordination, operational follow-up, and practice support.
Request an
AI Notes Trial
See how DENmaar AI Notes can help your clinicians reduce documentation time while improving
Request a demonstration or pilot program today.
Request Information
TESTIMONIALS
WHAT OUR CLIENTS SAY
On behalf of everyone at Meadowlark Counseling Services, I want to extend our sincere thanks for the continued improvements you and your team have made to the DENMaar EMR platform. We have been consistently impressed with both the functionality and user-friendly design of the system, which has made a meaningful difference in our day-to-day operations. The intuitive layout and ease of use have allowed our staff to spend less time navigating the system and more time focusing on client care. The regular updates and enhancements reflect your commitment to meeting the evolving needs of providers in the behavioral health and substance use treatment fields. We genuinely look forward to the new features introduced each month and appreciate how responsive the platform has been to the demands of clinical workflows. We have been so pleased with our experience that we’ve taken the opportunity to recommend DENMaar to other professionals in Pennsylvania who are working in the SUD field. Thank you again for your ongoing support and partnership. We are grateful to be working with a company that truly understands the needs of its users. KIndly, Becky Parks on behalf of the entire team at Meadowlark Counseling Services
I referred one of my colleagues Dr Aaron to you he is just starting g his psychology private practice and looking at where to start. I told him hands down you guys are the best billers and have a great EMR and team. He said he reached out just wanted to let you know!
FANTASTIC job keeping things rolling along with any and all of our billing concerns as well as responding to other issues which may well have been out of your wheelhouse. We are VERY grateful to have you and the crew in our corner.
I appreciate you all so much and DENmaar has been such a blessing Donna to our overall operations and success as an expanding company—allowing us to ultimately operate more efficiently, get our claims paid more consistently, ad stay on top of the critical credentialing piece, among other things. Teamwork does in fact, make the dream work. I’ll loop Chris/Isabella in on this message thread too, as I want All of your team to be aware of how much we appreciate our working relationship with DENmaar
Thank you for your diligence!! I appreciate it so much. Thank you Edwina…
Thank you so much Amy! I will be referring to DENmaar as often as I am asked about credentialing services.
Our Latest Blogs
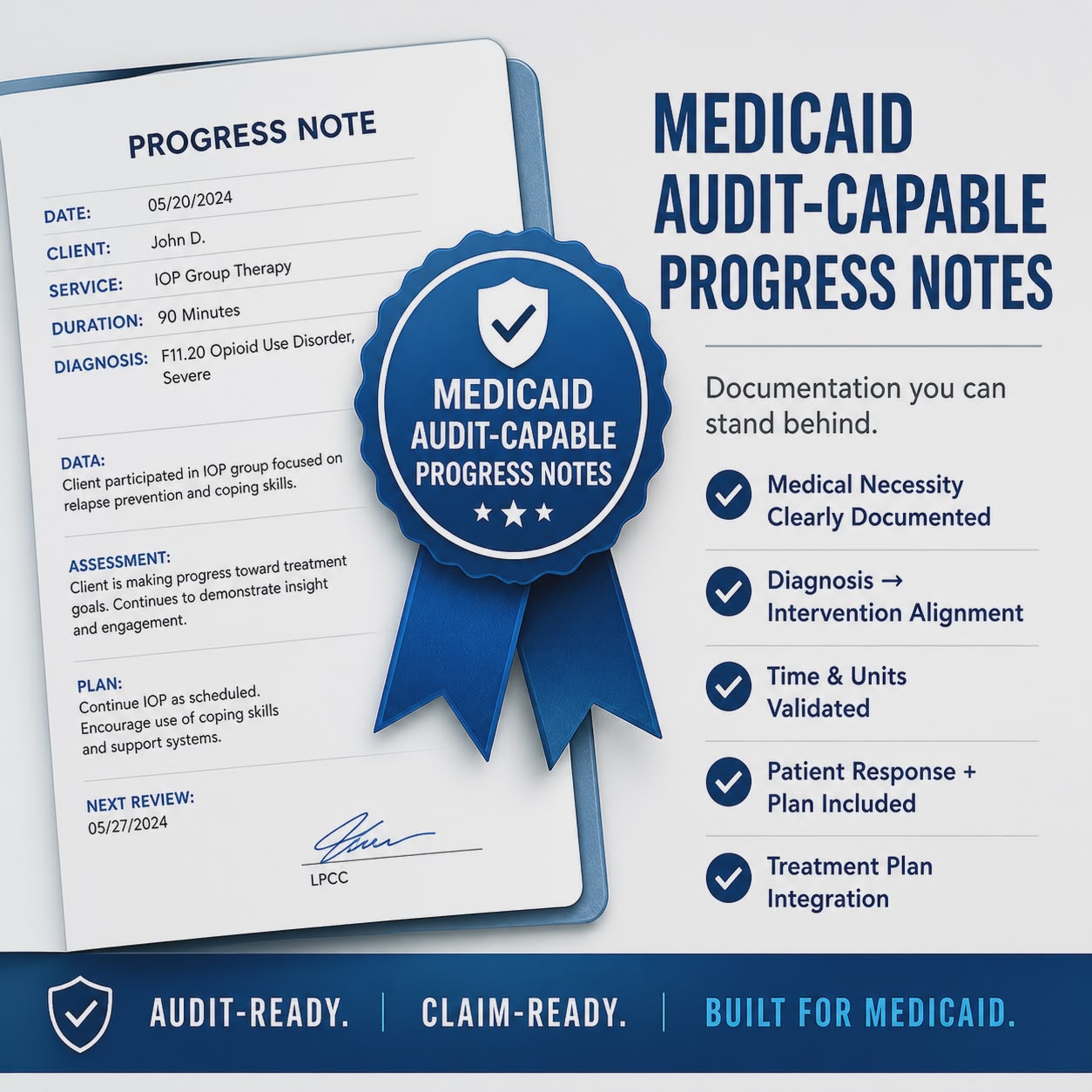
Why We Took Our Time to Build the Best Medicaid Focused Progress Notes
In behavioral health, progress notes are often treated as a formality.
- Something to complete.
- Something to store.
- Something to “get done.”
That approach is exactly why so many practices struggle with denials, audits, and inconsistent revenue.
We took a different path. We slowed down and built progress notes the right way.
The Problem: Most Progress Notes Aren’t Built for Medicaid
Medicaid is not forgiving.
Unlike many other payers, Medicaid programs expect:
- Clear medical necessity
- Tight alignment between diagnosis, intervention, and outcome
- Accurate time and unit reporting
- Consistency across providers and services
- Documentation that supports program-level care such as IOP, SUD, and community-based services
The issue isn’t that clinicians don’t know how to document. It’s that most systems don’t guide them to do it in a way that holds up under scrutiny.
That gap creates:
- Denials
- Recoupments
- Audit exposure
- Revenue leakage
This is one reason many organizations struggle with Medicaid billing behavioral health workflows and long-term compliance.
Our Approach: Documentation as a System, Not a Template
We didn’t start with templates. We started with the full lifecycle:
Scheduler → Session → Note → Daysheet → Claim → Payment
Then we asked a simple question:
What does the note need to contain to ensure the claim gets paid and survives an audit?
And that changed everything.
By integrating documentation directly into behavioral health revenue cycle management workflows, the system supports both compliance and reimbursement performance.
What We Built Differently
1. Structured for Medical Necessity
Every note enforces:
- Diagnosis linkage
- Symptom documentation
- Targeted interventions
- Patient response
- Forward plan
Not as optional fields, but as a guided clinical workflow.
This creates stronger behavioral health compliance and improves Medicaid behavioral health reimbursement outcomes.
2. Aligned With Billing Logic
Clinical documentation and billing cannot be separate systems.
Our notes are built to reflect:
- Service requirements
- Time thresholds and unit logic
- Program and payer expectations
This creates what we call Claims Hygiene, which helps generate clean claims behavioral health workflows before claims are ever submitted.
Integrated documentation also supports RCM for behavioral health by reducing rework and denied claims.
3. Consistency Across Providers
In multi-provider practices, inconsistency leads to risk.
We designed notes to:
- Standardize documentation quality
- Guide providers without slowing them down
- Reduce variability that leads to denials or audit issues
This is especially important for organizations using therapy practice management software and managing multiple clinicians across locations.
4. Built for Real Medicaid Workflows
We didn’t design for ideal scenarios. We designed for reality:
- Multiple services in a single day
- Group and individual sessions
- Program-based care such as IOP, SUD, ACT, and more
- State-specific requirements
This is where most systems break.
We built for it from the start.
Unlike traditional systems, modern behavioral health EHR platforms must support real Medicaid workflows tied directly to billing and operational logic.
The Result: Real World Validation
During a recent Medicaid site visit, a state representative reviewing one of our partner practices said:
“These are the best progress notes I’ve seen.”
That’s not marketing language.
That’s what happens when documentation is engineered with compliance, billing, and clinical care in mind at the same time.
This level of structure is critical for practices managing psychiatry billing Medicaid, substance use treatment workflows, and complex behavioral health programs.
Why This Matters
Progress notes are not just records. They directly impact:
- Revenue through clean versus denied claims
- Compliance and audit readiness
- Operational efficiency with less rework and fewer corrections
When documentation and billing are disconnected, practices often lose 10–20% of potential insurance revenue.
When they’re aligned, performance improves across the board.
Learn how integrated systems improve outcomes through AI behavioral health billing and clean claims workflows and connected documentation systems.
Where This Is Going
This foundation enables what comes next:
- AI-assisted notes that are actually audit-ready
- Measurement-Based Care integrated directly into documentation
- Diagnosis-to-intervention mapping
- Real-time validation before claims submission
The future isn’t faster note-taking.
It’s smarter, enforceable documentation that drives outcomes.
This is where AI progress notes and AI documentation for behavioral health become valuable when integrated into the clinical and billing workflow.
Final Thought
We didn’t rush this.
Because in Medicaid, shortcuts don’t show up immediately. They show up later in denials, audits, and lost revenue.
So we took our time.
And built progress notes that hold up under pressure.
Practices looking for scalable systems should evaluate how their psychiatry EHR and behavioral health billing workflows connect documentation, compliance, and reimbursement into one operational system.
Explore more about the benefits of behavioral and mental health billing services at DENmaar.
Frequently Asked Questions
Why are Medicaid progress notes important in behavioral health?
Medicaid progress notes support medical necessity, billing compliance, audit readiness, and accurate reimbursement. Poor documentation often leads to denials and revenue leakage.
How do AI progress notes improve behavioral health billing?
AI progress notes help standardize documentation, improve coding alignment, support claims hygiene, and reduce billing errors before claim submission.
What is claims hygiene in behavioral health billing?
Claims hygiene refers to creating accurate, audit-ready claims by aligning documentation, diagnosis, coding, eligibility, and billing workflows before submission.
How does structured documentation reduce denials?
Structured documentation ensures that required billing and compliance elements are captured consistently, reducing claim rejections, denials, and audit exposure.
What should a behavioral health EHR support for Medicaid billing?
A behavioral health EHR should support diagnosis linkage, time and unit validation, payer-specific workflows, AI documentation, and integrated revenue cycle management.

What Psychiatrists Should Actually Look for in an EHR And Why Most Platforms Fall Short
When psychiatrists evaluate an EHR, the checklist is usually the same:
- Documentation templates
- E-prescribing
- Scheduling
- Telehealth
- Patient portal
- Measurement-based care
- Reporting
On paper, most systems claim to offer all of this.
In reality, very few deliver it in a way that actually supports how a psychiatry practice operates, especially once you move beyond a solo provider into a multi-provider, insurance-based model.
This is where the gap starts to show.
The Core Problem: Fragmented Systems in Behavioral Health EHRs
Most behavioral health EHR platforms, including many mental health EHR software solutions, were not designed as operational systems. They are documentation tools with add-ons.
What that leads to:
- Documentation exists separately from billing
- Scheduling is disconnected from clinical workflow
- Measurement-based care is bolted on, not integrated
- Revenue cycle issues surface after claims are submitted
- Providers carry the burden of figuring it out across systems
For a psychiatrist running or joining a growing practice, this creates friction everywhere.
To understand how system gaps impact performance, see how structural instability in behavioral health practices is reshaping operations.
What a Psychiatry-Centered Behavioral Health EHR Should Actually Do
If you look at the workflow from intake to session to documentation to billing to follow-up, the system should function as a single loop.
Here’s what that means in practical terms:
1. Documentation That Drives the Entire Workflow
Psychiatric documentation shouldn’t just be a note.
It should:
- Capture DSM-5 diagnoses in a structured way
- Include MSE and risk assessment components
- Feed directly into billing logic such as CPT, units, and modifiers
- Connect to treatment planning and measurement-based care
Modern systems using AI progress notes for behavioral health and AI documentation for behavioral health can assist here, but only if grounded in structured clinical data, not just free text generation.
2. Measurement-Based Care That Isn’t an Afterthought
Most platforms include tools like PHQ-9 or GAD-7.
Very few actually integrate them.
A true system should:
- Be part of intake and ongoing care
- Flow into progress notes automatically
- Track trends over time
- Inform treatment decisions
This is critical for behavioral health compliance and payer expectations.
3. Scheduling That Acts as a Revenue Control Point
Scheduling isn’t just calendar management.
It should:
- Trigger eligibility and benefits checks
- Flag authorization issues before sessions occur
- Drive documentation workflows
- Feed clean data into billing
If scheduling is passive, errors show up downstream in claims and impact behavioral health revenue cycle management.
4. E-Prescribing That Fits Psychiatric Workflows
EPCS is now expected, but usability matters more than availability.
For psychiatry:
- Controlled substance workflows must be efficient
- Medication history should be easily accessible
- Integration with documentation is critical
If prescribing is clunky, it slows down the entire session.
5. Telehealth That Feels Native
Telehealth should not feel like a separate system.
It should:
- Launch directly from the schedule
- Tie into session tracking
- Feed into documentation automatically
- Be simple for patients
6. Patient Portal That Actually Engages Patients
A portal should do more than store forms.
It should:
- Handle intake and e-signatures
- Deliver rating scales
- Support secure messaging
- Feed structured data into the workflow
Otherwise, staff re-enters everything manually.
7. Multi-Provider and Supervision Workflows
As soon as a practice grows, complexity increases.
The system should support:
- Multiple providers with role-based access
- Supervision structures
- Shared visibility across teams
- Standardized workflows
This is where most therapy practice management software systems break down.
8. Reporting That Connects Clinical and Financial Data
Basic reporting isn’t enough.
You need visibility into:
- Patient volume and utilization
- No-show patterns
- Provider productivity
- Claims performance and revenue trends
This is where clinical operations intersect with behavioral health billing services and revenue.
The Missing Layer: Revenue Cycle Integration
This is the piece most psychiatrists underestimate.
Documentation, scheduling, and billing are not separate functions.
They are interdependent.
If your system does not:
- Validate insurance early
- Enforce clean documentation
- Align notes with billing requirements
- Monitor claims performance
You will lose revenue, even if everything looks fine.
Explore how claims hygiene in behavioral health billing improves clean claims behavioral health performance.
For deeper insight into integrated systems, review behavioral health billing services and AI-driven revenue cycle management.
Where the Industry Is Going
Behavioral health is moving toward:
- Measurement-based care as a standard
- Greater payer scrutiny
- Integrated team-based care
- Automation in documentation and billing
The EHR is no longer just a record system.
It’s becoming the operating system of the practice.
Modern platforms like behavioral health EHR systems and DENmaar are designed to unify clinical and financial workflows.
Final Thought
If you’re evaluating platforms, don’t just ask:
Does it have this feature?
Ask:
How does this feature connect to everything else in the system? Because in psychiatry, efficiency and revenue don’t come from isolated tools. They come from how well the entire workflow is integrated.
Frequently Asked Questions
What is the best EHR for psychiatry practices?
The best psychiatry EHR is one that integrates documentation, scheduling, and billing into a unified system, supports AI documentation, and improves clean claims and revenue cycle management.
Why do most behavioral health EHRs fail at billing?
Most systems treat billing as an add-on instead of integrating it into clinical workflows, leading to errors, denials, and lost revenue.
How does AI improve behavioral health documentation?
AI helps structure notes, align documentation with billing requirements, and improve accuracy, especially when combined with systems like AI progress notes.
What is claims hygiene in behavioral health?
Claims hygiene ensures that all upstream data such as documentation, eligibility, and coding are correct before submission, leading to higher clean claim rates and fewer denials.
Why is revenue cycle management important in psychiatry?
Effective RCM ensures accurate claims, faster reimbursements, and improved financial stability, especially for Medicaid and insurance-based psychiatry practices.
The Biggest Threat to Behavioral Health Practices Isn’t What You Think
Why Structural Instability Is Becoming the Real Risk in Behavioral Health
Most conversations about behavioral health focus on the obvious:
- Staffing shortages
- Burnout
- Reimbursement rates
- Access to care
All real. All important.
But they’re not the biggest threat.
The Real Problem: Structural Instability
Behavioral health practices today are operating in an environment that is becoming:
- Less predictable
- More regulated
- More fragmented
And it’s happening fast.
This isn’t a single issue—it’s a convergence of forces that are reshaping how practices operate.
Medicaid Is Becoming Less Reliable
Behavioral health is heavily dependent on Medicaid.
And right now, Medicaid is changing:
- Eligibility requirements are tightening
- Coverage is fluctuating more frequently
- Provider audits and revalidation are increasing
For practices, this means:
- Patients who were covered last month may not be today
- Eligibility can no longer be assumed
- Claims are more likely to fail due to coverage gaps
This introduces something most practices aren’t designed for:
Constant uncertainty at the point of care
Modern behavioral health EHR software should verify eligibility in real time and reduce Medicaid claims friction.
Funding Is No Longer Stable
Federal and state behavioral health funding has become unpredictable.
Programs expand—and then contract.
Budgets shift.
Policies reverse.
Practices that relied on:
- Grants
- State programs
- Supplemental funding
Are now forced to depend more heavily on:
Consistent, accurate insurance reimbursement
That’s a problem if your system isn’t built for it.
This is why strong mental health billing services and revenue cycle systems matter more than ever.
AI Is Rising—But Not Where It Matters Most
There’s a lot of noise around AI in mental health.
- AI therapists
- Chatbots
- Digital companions
But the real opportunity isn’t replacing clinicians.
It’s fixing operations.
The practices that benefit from AI won’t be the ones using it to simulate therapy.
They’ll be the ones using it to:
- Improve documentation
- Enforce workflows
- Prevent billing errors
- Optimize revenue
Solutions like AI behavioral health billing systems and AI progress notes are where measurable ROI happens.
Compliance Pressure Is Increasing
Behavioral health has historically been loosely structured compared to other areas of healthcare.
That’s changing.
There is growing scrutiny around:
- Credentialing
- Documentation
- Billing accuracy
This means:
- More audits
- More denials
- Greater financial risk for mistakes
The margin for error is shrinking.
Practices need stronger behavioral health compliance systems and provider credentialing controls.
The System Most Practices Use Can’t Handle This
Here’s the underlying issue:
Most practices are still operating with disconnected tools:
- An EHR
- A billing service
- A scheduler
- Manual processes in between
These systems were built for a simpler environment.
They don’t:
- Adapt in real time
- Enforce correct workflows
- Prevent errors before they happen
So when complexity increases, performance breaks down.
Many of these failures are caused by poor claims communication workflows and fragmented processes.
What Needs to Change
The industry doesn’t need another EHR.
It needs a system that functions as a behavioral and financial control layer.
A system that:
- Validates insurance before the visit
- Detects carve-outs and special workflows
- Confirms authorization requirements
- Aligns documentation with billing logic
- Prevents invalid claims before submission
This is the foundation of claims hygiene in behavioral health billing.
Why the Scheduler Becomes the Most Important Part of the System
If there’s one place to fix this, it’s not billing.
It’s before the session even starts.
At the point of scheduling and check-in.
This is where:
- Coverage can be verified
- Risks can be identified
- Patients can be informed
- Decisions can be made
Once the session happens, the opportunity to prevent errors is gone.
A modern therapy practice management software platform should make scheduling financially intelligent.
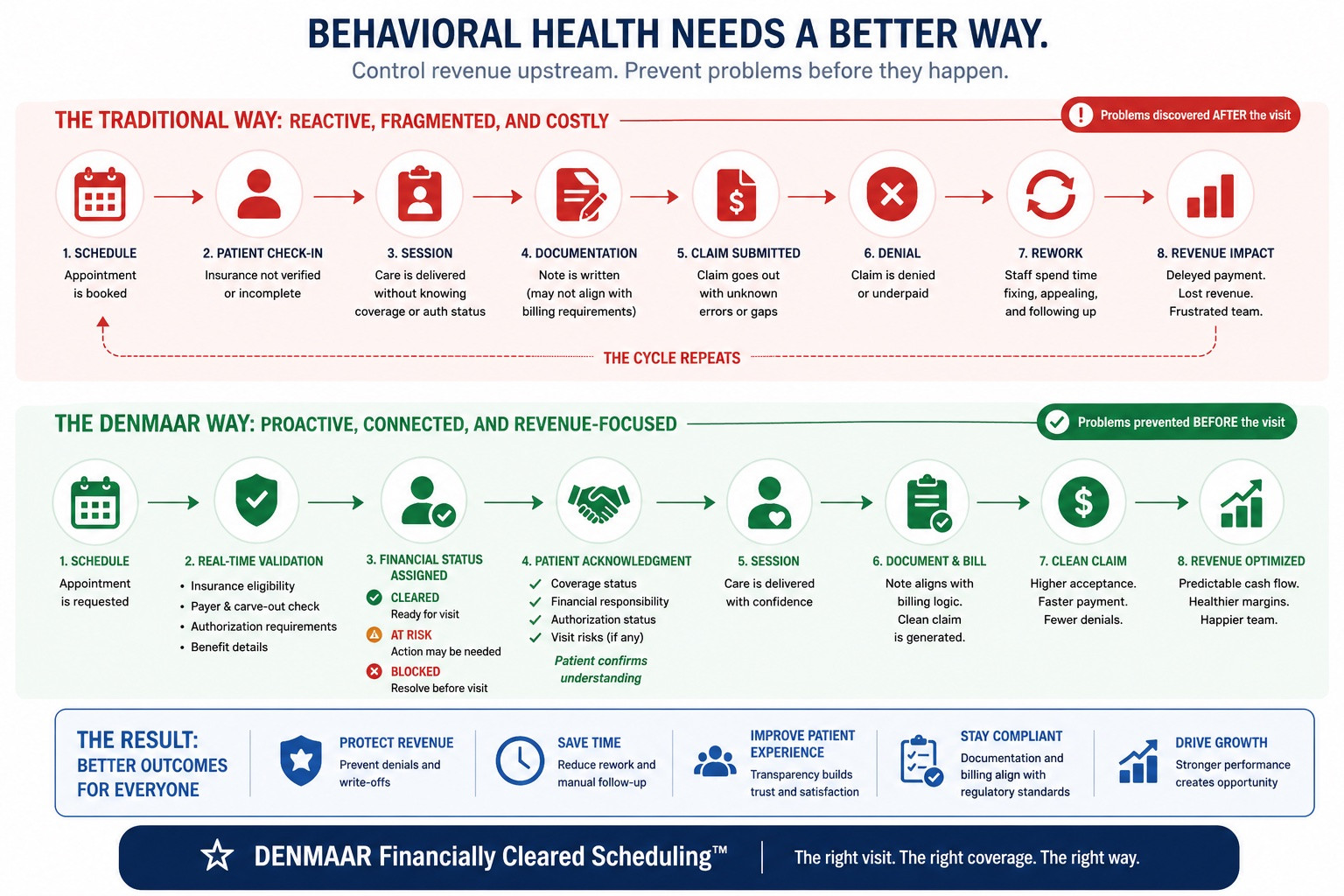
A New Standard: Financially Cleared Scheduling
Forward-thinking practices are beginning to adopt a new approach:
Every appointment must be financially validated before care is delivered.
That means:
- Insurance is confirmed
- Authorization is verified
- The correct billing pathway is identified
- The patient acknowledges their financial responsibility
If something isn’t right, it’s addressed before the visit—not after the denial.
Learn how integrated systems like DENmaar make this possible.
The Result
Practices that operate this way see:
- Fewer denials
- Higher clean claim rates
- Faster reimbursement
- More predictable cash flow
Not because they work harder—but because their system enforces the right behavior.
This is true behavioral health revenue cycle management.
Final Thought
Behavioral health isn’t just facing challenges.
It’s entering a more complex, less forgiving operating environment.
The practices that succeed won’t be the ones that react better.
They’ll be the ones that:
Control the system upstream before problems ever occur.
Frequently Asked Questions
What is the biggest threat to behavioral health practices today?
The biggest threat is structural instability caused by Medicaid uncertainty, fragmented billing systems, compliance pressure, and poor revenue workflows.
Why are Medicaid claims harder for behavioral health practices?
Frequent eligibility changes, carve-outs, audits, and authorization complexity make Medicaid behavioral health claims harder to manage.
What is financially cleared scheduling?
It means validating insurance, authorizations, payer routing, and patient responsibility before the appointment occurs.
How can AI help behavioral health organizations?
AI can improve documentation, automate claims hygiene, reduce denials, and optimize billing workflows.
Why do disconnected EHR and billing systems fail?
Because they do not share data efficiently, prevent upstream errors, or adapt quickly to payer and compliance changes.
Our Partners
Ready to get started?
Feel free to reach out if you have any questions.