Multidisciplinary Care, Dual Claim Systems, and the Rise of Claims Hygiene
Behavioral health is changing.
Over the past decade, the industry has expanded beyond traditional outpatient therapy into a much broader continuum of care. Today’s practices increasingly include multiple service lines:
- Outpatient therapy
- Psychiatry and medication management
- Substance use disorder (SUD) treatment
- Intensive outpatient programs (IOP)
- Partial hospitalization programs (PHP)
- Community-based services
- Residential programs such as ASAM 3.1
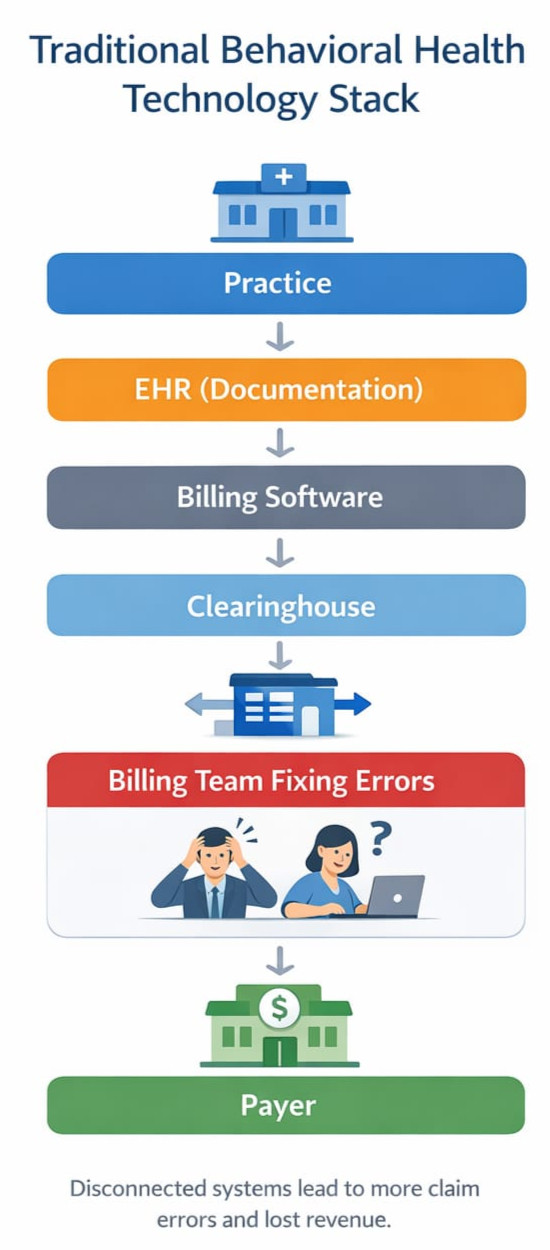
Yet the technology supporting many of these organizations still assumes a simple model: one provider, one discipline, one claim type.
That assumption no longer holds.
Modern behavioral health organizations require systems designed around multiple disciplines, multiple billing frameworks, and increasingly complex payer rules.
The practices that understand this shift are building something fundamentally different.
For many organizations, adopting a modern behavioral health EHR platform and integrated behavioral health revenue cycle management approach is the first step toward solving these challenges.
The Multidisciplinary Behavioral Health Organization
The most resilient behavioral health organizations today are not single-service clinics.
They are multidisciplinary systems of care.
A single organization might include:
- Licensed therapists
- Psychiatrists and psychiatric nurse practitioners
- SUD counselors
- Case managers
- Community support specialists
- Residential program staff
Each discipline introduces different documentation standards, payer expectations, and billing structures.
A therapy session may be billed as CPT 90837, while case management could use T1016, and an intensive outpatient day might involve a facility-based service with entirely different billing rules.
Trying to run this ecosystem on software designed only for therapy quickly creates friction.
This is where the distinction between professional claims and facility claims becomes critical.
Many organizations discover they are losing significant insurance revenue due to billing inefficiencies, something explored in detail in this analysis of how providers lose 10–20% of insurance revenue due to revenue cycle gaps.
CMS-1500 vs UB-04: Two Claim Worlds in Behavioral Health
Behavioral health providers often operate across two fundamentally different claim systems.
Understanding CMS 1500 vs UB 04 billing is essential for accurate Medicaid behavioral health reimbursement and clean claims.
CMS-1500 (Professional Claims)
Used for services delivered by individual clinicians such as:
- Therapy sessions
- Psychiatric evaluations
- Medication management
- Individual counseling
These claims are built around:
- CPT / HCPCS procedure codes
- Rendering provider information
- Service units and modifiers
This is the traditional model most EHRs support.
But it is only half the story.
UB-04 (Facility Claims)
Programs such as IOP, PHP, residential treatment, and some SUD services may require facility billing.
These claims rely on a completely different structure:
- Revenue codes
- Facility identifiers
- Program-level billing logic
- Episode-based service tracking
Many organizations running these services discover that their EHR cannot properly support UB-04 workflows.
As a result, staff often build manual workarounds, spreadsheets, and external billing processes.
The operational cost of this fragmentation is enormous.
This is why many providers adopt specialized behavioral health billing services designed for complex Medicaid and multi-program organizations.
The Hidden Problem: Claims Hygiene in Behavioral Health Billing
Even with the right claim format, most behavioral health revenue cycles struggle with something far more basic.
Data integrity.
We call this claims hygiene in behavioral health billing.
Claims hygiene refers to the accuracy and completeness of the information required to produce a clean claim:
- Correct insurance identification
- Accurate payer routing
- Valid provider credentials
- Proper service coding
- Diagnosis linkage
- Authorization verification
- Clean eligibility data
When these elements are wrong or incomplete, claims fail.
The result is familiar to many organizations:
- Rising denial rates
- Aging receivables
- Administrative overload
- Lost revenue
Improving claims hygiene is often the fastest way to increase revenue without seeing a single additional patient.
Where Most Behavioral Health Systems Fail
Many EHR platforms were originally designed for small outpatient therapy practices.
They assume a simple model:
One clinician
One note
One claim
But multidisciplinary behavioral health organizations operate in a very different reality.
They need systems capable of supporting:
- Multiple clinical disciplines
- CMS-1500 professional claims
- UB-04 facility claims
- Complex Medicaid program structures
- Integrated behavioral health revenue cycle management workflows
Without this architecture, billing becomes an afterthought rather than an integrated system.
Organizations increasingly turn to purpose-built platforms like DENmaar EHR, designed specifically for behavioral health compliance, Medicaid billing workflows, and multi-program organizations.
The Future: Integrated Behavioral Health Operating Systems
The next generation of behavioral health platforms will not separate clinical documentation from revenue cycle management.
Instead, they will treat documentation, scheduling, and billing as a single operational system.
This means:
- Services mapped to claim type (CMS-1500 or UB-04)
- Documentation structured to support billing requirements
- Eligibility and payer data captured early in the workflow
- Claims validated before submission
When this approach is implemented correctly, organizations see dramatic improvements:
- Higher clean claim rates
- Faster reimbursements
- Reduced administrative workload
- More predictable revenue
Modern platforms are also introducing AI progress notes for behavioral health, allowing clinicians to automate documentation while maintaining compliance with billing requirements.
A System Designed for the Real Behavioral Health Market
The behavioral health industry is not simple.
It spans therapy, psychiatry, substance use treatment, residential care, and community-based services.
Technology must reflect that complexity.
The organizations that thrive in the next decade will be those that build systems around three principles:
- Multidisciplinary care delivery
- Support for both CMS-1500 and UB-04 claim structures
- Operational discipline around claims hygiene
This is not just a billing strategy.
It is a new operating model for behavioral health.