And Why Most Practices Are Fixing It Too Late
Most behavioral health practices think claim problems start in billing.
They don’t.
By the time a claim reaches a billing team, the outcome is already largely determined. Denials, rejections, underpayments are usually symptoms of upstream breakdowns that occurred days or weeks earlier inside the EHR.
We call this claims hygiene.
And if it is not engineered into your system, no amount of billing follow-up will fully fix it.
For a deeper breakdown of structured prevention, see claims hygiene in behavioral health billing.
Claims Hygiene Defined
Claims hygiene is the condition where every step before claim submission is structurally aligned to produce a payable claim by default.
That includes:
- Correct payer identification, especially mental health carve-outs
- Authorization-aware scheduling
- Time and unit accurate documentation
- Diagnosis logic that matches the service performed
- Day sheet logic that enforces payer rules before release
When these elements are clean and coordinated, billing becomes simple.
When they are not, billing becomes damage control.
This is not just a billing workflow. It is behavioral health revenue cycle management designed upstream inside the EHR.
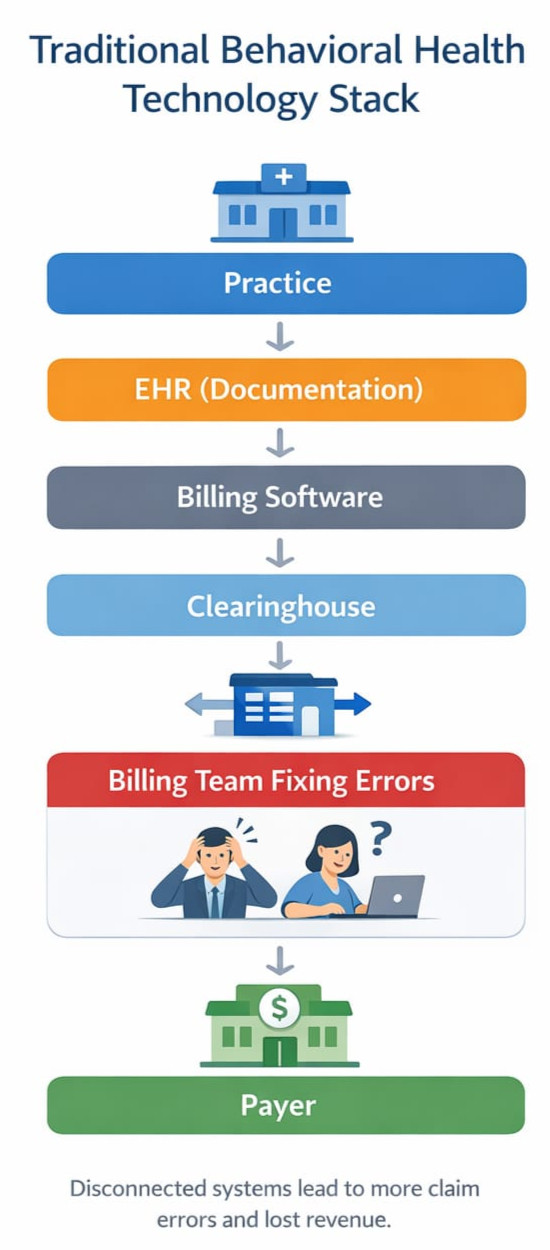
Where Claims Actually Break (Upstream, Not in Billing)
In behavioral health billing, especially in Medicaid billing behavioral health environments, claim failure usually originates in one of four places:
1. Scheduling Without Payer Logic
Appointments are booked without confirming:
- The correct mental health payer
- Whether the service requires authorization
- Whether the provider is credentialed for that payer or program
Once the visit happens, the financial risk is already locked in.
Without integrated provider credentialing and insurance credentialing services awareness, scheduling becomes financially blind.
2. Documentation That Is Clinically Fine but Billing Unsafe
Notes often fail not because they are poor clinically, but because:
- Time thresholds do not match billed units
- Services rendered do not align with diagnosis logic
- Required elements for specific CPT or HCPCS codes are missing
Billing teams cannot fix documentation that was never structured correctly.
This is where structured AI documentation for behavioral health, including AI powered progress notes, becomes critical. Documentation must be payer aware, not just clinically complete.
3. Day Sheets That Do Not Enforce Rules
The day sheet is the last gate before claim submission and in many systems, it is passive.
If a day sheet allows:
- Invalid unit counts
- Missing authorizations
- Diagnosis and code mismatches
Then the system is allowing bad claims to exist.
A strong behavioral health EHR and mental health EHR software platform should enforce payer logic before claims are generated
4. Billing Teams Forced Into Manual Recovery
This is where most practices focus, but it is already too late.
At this stage, billing teams are:
- Correcting errors they did not create
- Appealing preventable denials
- Chasing missing information retroactively
This is not revenue cycle management. It is revenue triage.
True behavioral health billing services should prevent these breakdowns before submission.
Why “Clean Claims” Is the Wrong Goal
Many platforms advertise clean claim rates, but that metric is misleading.
A claim can be clean to a clearinghouse and still:
- Hit the wrong payer
- Violate MCO rules
- Fail authorization requirements
- Deny weeks later
True clean claims in behavioral health are payer true, service true, and rule true before submission ever happens.
This is especially critical in Medicaid claims behavioral health, psychiatry billing Medicaid, and substance use treatment billing environments where CMS 1500 versus UB 04 differences and managed care carve-outs matter.
Why Scaling Makes This Worse Fast
At 1 to 2 providers, errors are survivable.
At 10 or more providers:
- Small inconsistencies become systemic revenue loss
- Training breaks down
- Manual checks do not scale
- Billing headcount grows without fixing root causes
This is why many practices hit a ceiling where revenue plateaus despite growing volume.
Scaling requires system enforced behavioral health compliance, not manual memory.
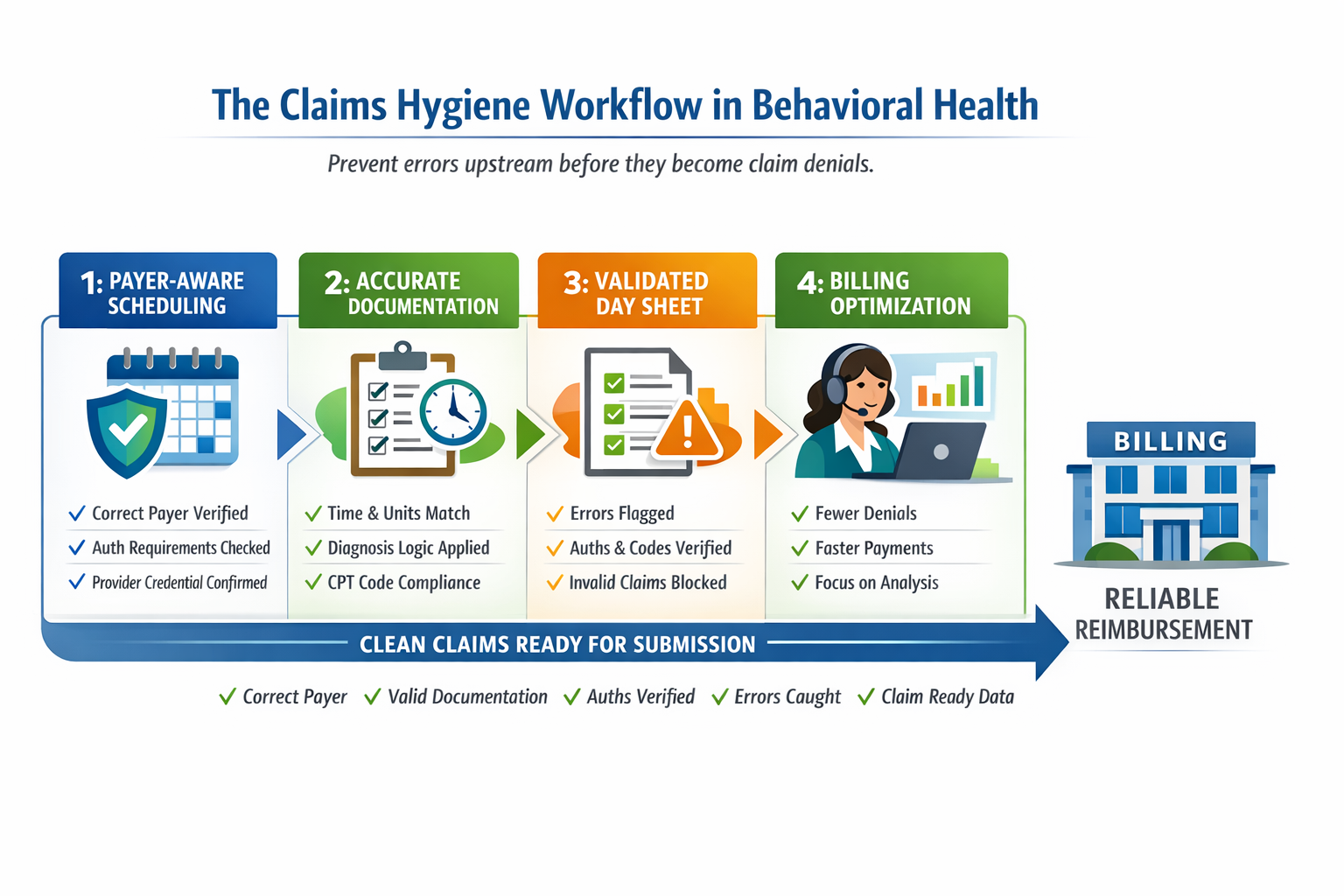
What Real Claims Hygiene Looks Like
In a hygienic system:
- Insurance verification identifies mental health carve-outs automatically
- Scheduling is constrained by authorization and credentialing reality
- Documentation enforces time, units, and service logic
- Day sheets block invalid claims by design
- Billing teams focus on optimization, not cleanup
When this is in place, practices typically see:
- Fewer rejections and denials
- Faster payment cycles
- Lower billing staff burnout
- 10 to 20 percent improvement in realized insurance revenue without adding patients
This is the difference between submitting claims and building a revenue safe behavioral health system.
The Core Insight
Claims hygiene is not a billing function.
It is a system design problem.
If your EHR allows bad data to flow freely, billing will always be reactive.
If your system enforces payer aware logic upstream, billing becomes predictable and scalable.
Learn more about system level prevention at DENmaar.
Final Thought
Most practices do not need better billers.
They need fewer preventable mistakes.
Claims hygiene is not something you fix after the fact.
It is something you engineer into the workflow.
That is the difference between submitting claims and building a revenue safe system.