Behavioral health practices often assume billing problems come down to staff performance. Claims get rejected, payments are delayed, and revenue fluctuates unpredictably. The typical conclusion is that the billing team needs better training or more oversight.
In reality, the problem usually starts much earlier in the system architecture.
Most behavioral health EHRs were never designed to support efficient behavioral health revenue cycle management. Billing was added later as an auxiliary feature rather than built into the clinical workflow itself. This structural issue creates ongoing problems that practices attempt to solve with more staff, more manual review, and more time spent chasing claims.
The result is predictable: lost revenue, administrative friction, and frustrated providers.
Modern organizations increasingly rely on integrated platforms like behavioral health EHR and mental health practice management software designed to align clinical workflows with billing accuracy and Medicaid reimbursement requirements.
The Structural Problem With Most EHRs
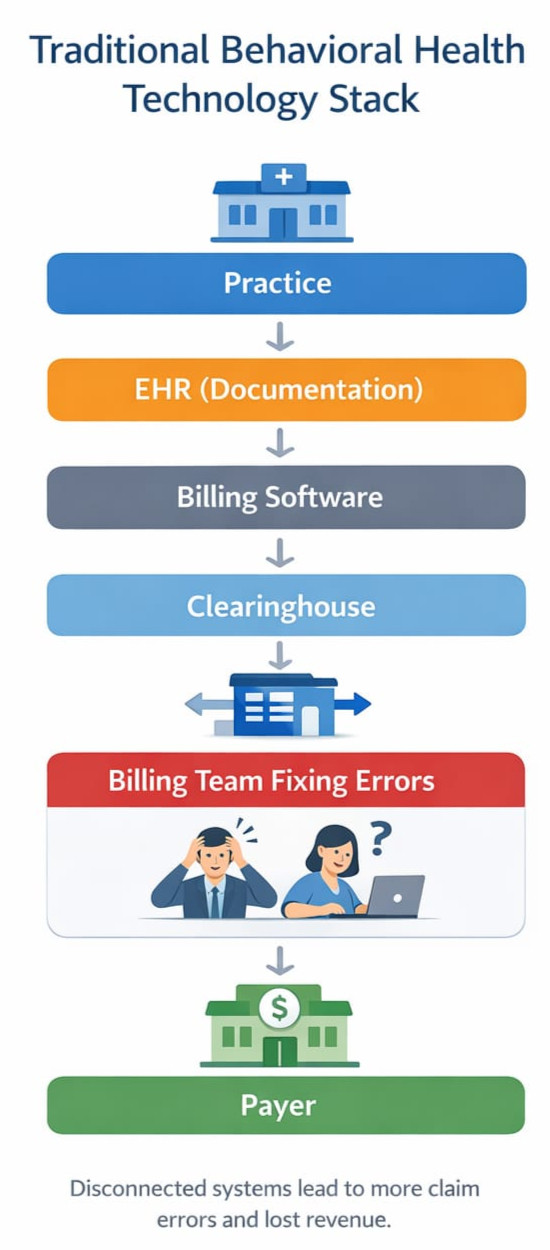
The traditional behavioral health technology stack looks something like this:
Practice → EHR → Billing Software → Clearinghouse → Billing Team
Each layer operates somewhat independently. Documentation is completed inside the EHR, then billing staff extract the information needed to generate claims. If documentation is incomplete, inconsistent, or coded incorrectly, the claim fails downstream.
This architecture introduces several common problems.
Documentation and Billing Are Disconnected
Clinical notes are written for clinical purposes, not claim validation. Important billing elements such as time requirements, service modifiers, or diagnosis linkage may not be captured correctly in the workflow.
Modern systems increasingly solve this problem through structured documentation and AI progress notes for behavioral health, ensuring that clinical documentation supports both care delivery and billing compliance.
Errors Are Discovered Too Late
In many systems, claim validation occurs only after the claim is generated and submitted. By that point, rejections or denials require additional staff intervention.
Eligibility and Payer Rules Are Separate From Clinical Workflow
Eligibility verification and payer specific requirements often live outside the EHR entirely. Front desk staff, clinicians, and billing teams operate with incomplete information about payer policies.
Claims Follow Up Becomes Labor Intensive
When problems occur, billing teams spend hours tracking down documentation errors, contacting payers, or correcting claims.
None of these problems are fundamentally about the billing staff.
They are system design problems.
The Real Cost of Fragmented Billing Systems
Behavioral health practices frequently underestimate how much revenue is lost through inefficient billing infrastructure.
Common revenue leakage points include:
- Incorrect or missing modifiers
- Mismatched documentation and CPT codes
- Eligibility verification failures
- Incorrect claim forms such as CMS-1500 vs UB-04
- Incomplete prior authorization tracking
- Delayed follow up on rejected claims
Across the industry, these issues typically reduce collected revenue by 10–20%.
Many organizations are unaware that behavioral health providers lose 10–20 percent of insurance revenue due to inefficiencies in billing workflows and claims management.
For many practices, that difference determines whether they are able to hire additional clinicians, expand services, or invest in better care infrastructure.
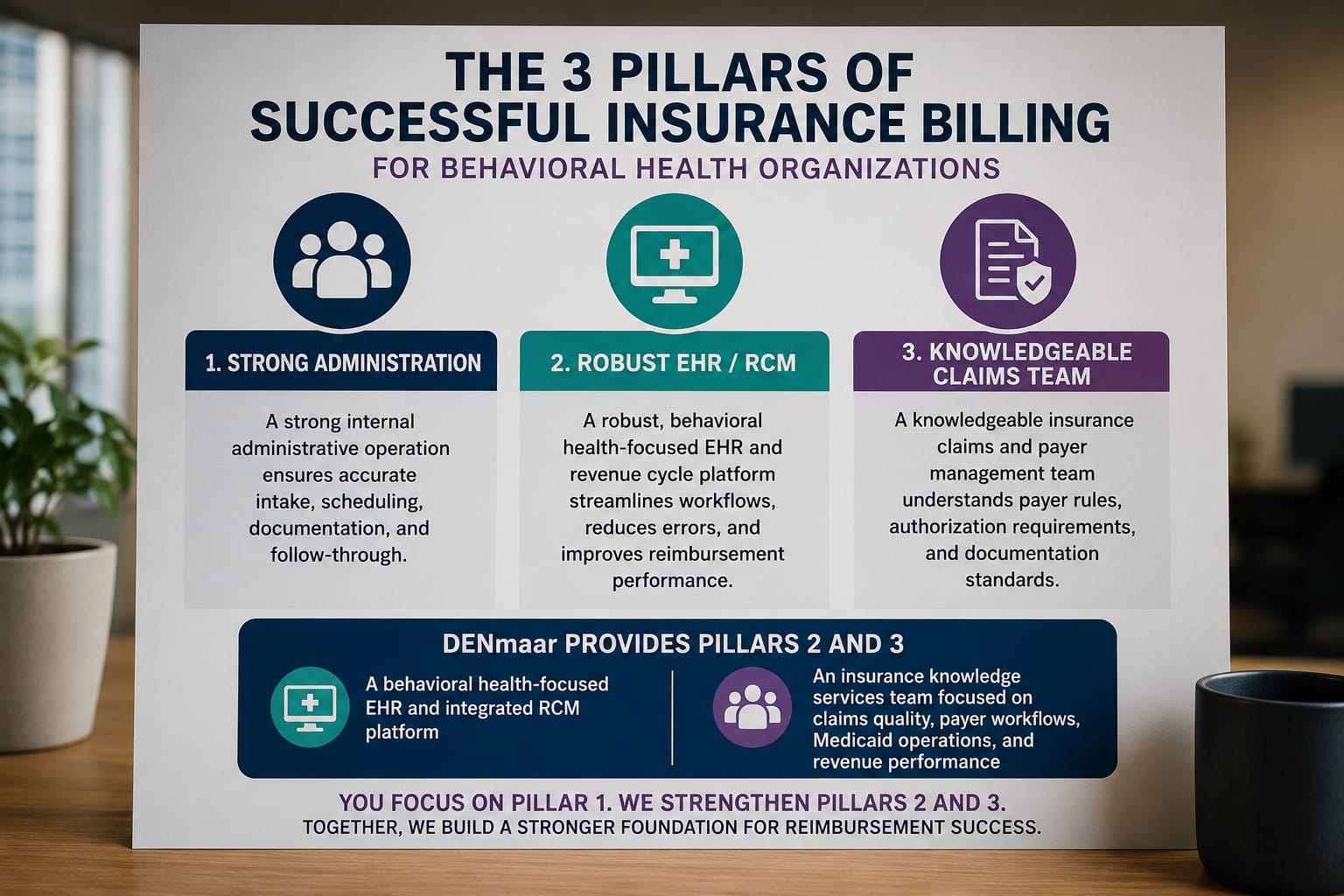
What a Billing-Optimized Behavioral Health EHR Looks Like
If billing performance depends on system architecture, the logical solution is to design the clinical system around revenue cycle integrity from the beginning.
A billing optimized behavioral health platform integrates several core elements directly into the workflow.
Documentation That Drives Coding
Clinical documentation should guide coding decisions rather than leaving coding entirely to billing staff. Structured note elements help ensure that required billing information such as time thresholds, service type, and diagnosis linkage is captured during the clinical encounter.
Integrated Eligibility and Payer Intelligence
Eligibility verification and payer rules should be visible within the system before services occur. This allows practices to confirm coverage, identify authorization requirements, and avoid preventable claim failures.
Pre Submission Claim Validation
Claims should be evaluated and scrubbed before submission to clearinghouses. Identifying errors upstream prevents the cycle of rejection, correction, and resubmission that slows revenue flow.
Maintaining strong claims hygiene in behavioral health billing is one of the most effective ways to improve clean claims rates and Medicaid reimbursement.
Continuous Claims Monitoring
Billing does not end at submission. Effective systems monitor claim status, identify payer responses, and intervene when issues arise.
Support for Multiple Billing Models
Behavioral health organizations increasingly operate across multiple service levels and billing structures. Systems must support both CMS-1500 professional claims and UB-04 institutional claims depending on the services provided.
Without this flexibility, practices are forced to maintain multiple disconnected systems.
Many organizations address this complexity through specialized behavioral health billing services and integrated revenue cycle management solutions.
Why This Matters for Behavioral Health
Behavioral health reimbursement is particularly complex compared with many other healthcare sectors.
Practices frequently operate across multiple disciplines including:
- Therapy
- Psychiatry
- Substance use disorder treatment
- Intensive outpatient programs (IOP)
- Community based services
- Case management
Each service category introduces different coding requirements, payer rules, and claim forms.
If billing logic is not integrated directly into the clinical infrastructure, the administrative burden grows rapidly as practices expand.
This is one reason many behavioral health organizations struggle to scale.
The Future of Behavioral Health Infrastructure
Over time, behavioral health technology will move away from isolated software tools toward integrated operating systems for practices.
In this model, documentation, billing, credentialing, communication, and analytics are connected within a unified platform.
Clinical workflow generates structured data that feeds directly into revenue cycle processes. Claims validation occurs automatically before submission. Eligibility, authorizations, and payer rules are continuously integrated into the system.
Platforms like DENmaar EHR are built around this concept, combining behavioral health documentation, billing workflows, and revenue cycle management into a single system.
The result is a much more stable and predictable revenue cycle.
The Results of an Integrated Approach
When billing architecture is built directly into the platform, claim performance improves dramatically.
At DENmaar, for example, practices operating within an integrated clinical and revenue cycle system currently achieve:
- 98.1% clean claims
- 1.47% rejected claims
- 0.32% denied claims
Those numbers place performance within the top tier of healthcare revenue cycle outcomes.
More importantly, practices using integrated systems typically experience 10–20% increases in insurance revenue simply by reducing claim friction and administrative leakage.
The Takeaway
When billing problems arise, it is easy to assume the issue lies with the billing team.
In many cases, the real cause is the technology architecture supporting the revenue cycle.
Behavioral health practices that want to grow sustainably need systems designed around billing integrity from the start rather than systems where billing is an afterthought.
As behavioral health services continue to expand and payer requirements grow more complex, billing optimized infrastructure will increasingly define which organizations succeed.
And which ones continue struggling with the same avoidable claim problems.