Turning Complex Care into Clean, Payable Claims
Artificial Intelligence is everywhere in healthcare right now.
But most of it is noise.
Chatbots. Auto notes. Surface level automation.
None of that solves the real problem behavioral health practices face:
How do you consistently turn complex, multidisciplinary care into clean, payable claims?
That is where AI actually matters.
Modern behavioral health EHR systems and behavioral health revenue cycle management platforms must focus on turning documentation into compliant claims that meet payer rules, Medicaid billing requirements, and behavioral health compliance standards.
The Real Use Case: Claims Intelligence, Not AI Features
AI is not most valuable in generating notes or answering phones.
It is most valuable when it acts as a real time enforcement and learning layer across your behavioral health revenue cycle management workflow.
Specifically:
- Before submission ensuring claims are correct
- After submission ensuring revenue is optimized
Everything else is secondary.
Systems that integrate behavioral health billing services, documentation, and payer rules directly into a unified platform like behavioral health EHR and mental health EHR software can dramatically improve claims accuracy and reimbursement performance.
1. Pre Submit: Where Revenue Is Won or Lost
Most revenue leakage happens before a claim is ever submitted.
Not because providers are not doing the work but because:
- Rules vary by payer
- Documentation does not map cleanly to billing
- Multidisciplinary workflows create inconsistencies
This is where AI delivers the highest ROI.
What AI Should Be Doing Pre Submit
A true system should function as a claims hygiene engine, enforcing standards across the behavioral health billing workflow.
Learn more about building claims hygiene in behavioral health billing.
- Time to Unit Validation
Ensuring session duration aligns with CPT codes such as 90837 vs 90834.
- Modifier Logic
Applying correct modifiers like 59 or XE based on context.
- Diagnosis to Service Alignment
Not just valid but likely to pay.
- Authorization Tracking
Matching authorized units to scheduled and documented services.
- Place of Service Accuracy
Telehealth versus in person versus facility based services mapped correctly per payer.
- UB04 vs CMS 1500 Routing
Determining the correct billing form based on service type, payer requirements, and facility structure.
This distinction between CMS 1500 vs UB 04 billing models is critical for organizations handling therapy, psychiatry, and facility services.
The Key Insight
This is not about replacing rules.
It is about managing rule complexity at scale across:
- Multiple disciplines
- Multiple payers
- Multiple program types
Organizations that invest in modern RCM for behavioral health infrastructure can dramatically reduce billing friction and increase Medicaid behavioral health reimbursement accuracy.
2. The Hidden Problem: Multidisciplinary Complexity
Most systems are built for one type of provider.
Behavioral health is not.
You are managing:
- Therapy
- Psychiatry
- Case management
- SUD, IOP, and facility services
Each with:
- Different documentation
- Different billing rules
- Different compliance requirements
Where AI Actually Wins
AI creates a translation layer between:
What happened clinically
What is billable
What will get paid
This is where most revenue is lost and where most systems fail.
Platforms that integrate documentation with billing such as AI powered progress notes for behavioral health help ensure clinical documentation aligns with payer requirements and CPT coding rules.
3. Post Submit: Where AI Becomes a Force Multiplier
Once claims are submitted, the problem changes.
Now it is not about correctness. It is about optimization.
What AI Should Be Doing Post Submit
- Denial Pattern Analysis
Identifying systemic issues instead of isolated denials. - Payer Behavior Modeling
Understanding which payers delay, deny, or underpay. - Follow Up Prioritization
Directing billing teams toward tasks that actually drive ROI. - Underpayment Detection
Comparing expected versus actual reimbursement across Medicaid, commercial payers, and facility claims.
Practices that use specialized behavioral health billing services integrated with AI systems gain far more visibility into payer performance and reimbursement trends.
Important Distinction
AI should not replace your billing team.
It should make your billing team exponentially more effective.
Modern therapy practice management software and mental health EHR systems should combine automation with human expertise to strengthen the behavioral health revenue cycle.
4. What AI Is NOT Good At
To be clear, there are areas where AI is overhyped:
- Fully autonomous payer calls
- Portal scraping at scale
- Static rule engines
- Generic note generation disconnected from billing
These approaches do not reduce denials.
They often increase them.
This is why many practices struggle when their technology stack separates documentation, billing, and revenue cycle management, a challenge explored in why many behavioral health EHR billing systems fail.
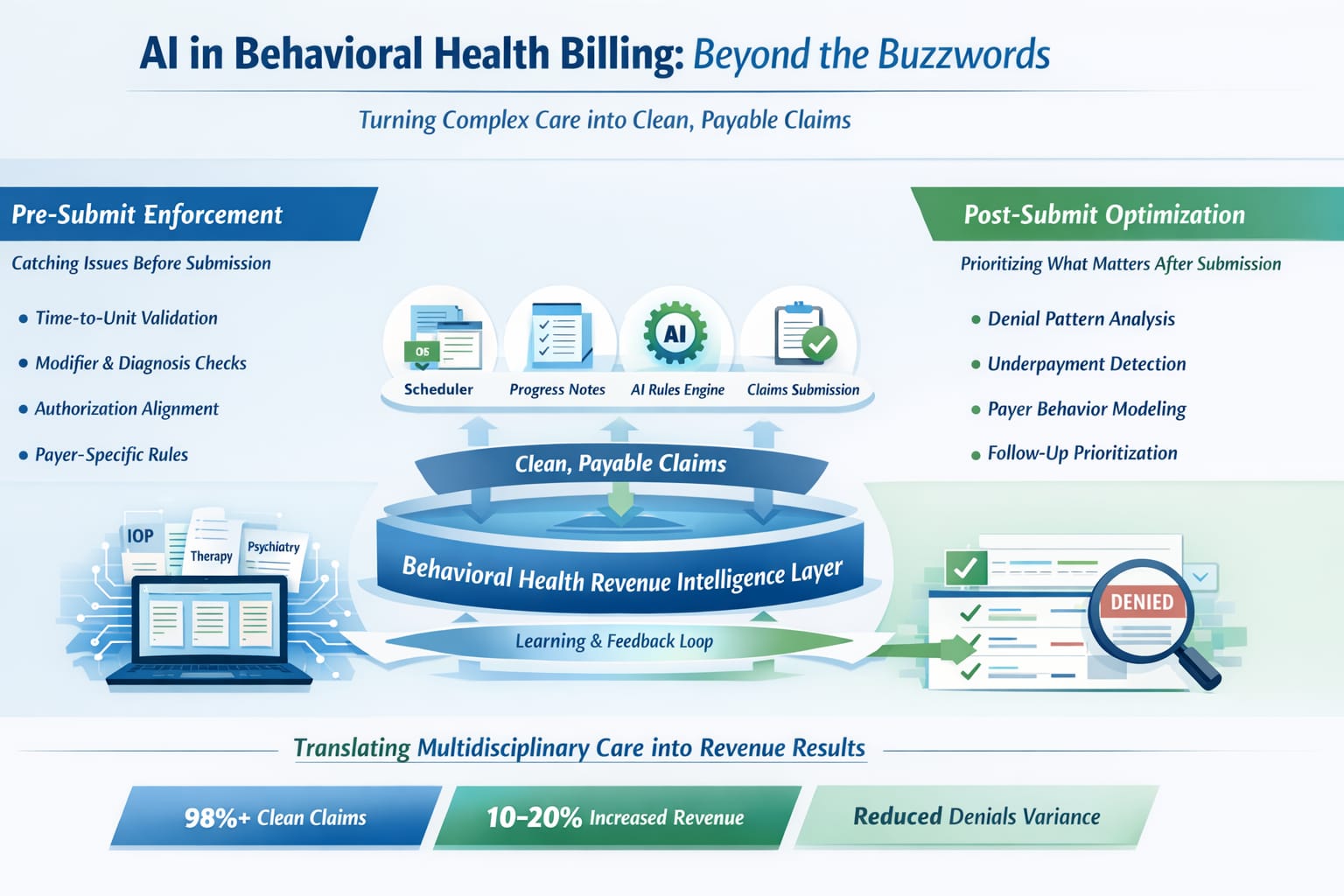
5. The Architecture That Actually Works
The future is not ‘AI tools’.
It is an integrated system:
- Scheduler
Sets expected billing reality. - Progress Notes
Confirm clinical and compliance reality. - Daysheet (Critical Layer)
AI answers:
Can this be billed?
Will this get paid?
- Claim Submission
Clean validated output. - Post Submit Engine
Learns → feeds back → improves system
This approach is known as preventative claims infrastructure, which focuses on preventing denials before they occur rather than fixing them later.
You can explore the full model of preventative claims infrastructure for behavioral health billing.
6. The Outcome: Measurable, Not Theoretical
When implemented correctly:
- 98% + clean claims
- Reduced denial variability across disciplines
- Faster onboarding of complex practices
- Less dependency on highly specialized billing staff
And most importantly:
A 10 to 20% increase in insurance revenue
Not by charging more.
But by capturing revenue that was already being earned and lost in complexity.
Organizations using integrated behavioral health revenue cycle management systems consistently outperform fragmented technology stacks.
Final Thought
AI in behavioral health is not about automation.
It is about enforcement and translation.
Turning multidisciplinary care into structured, compliant, payable claims every time.
That is where the real value is.
At DENmaar, this intelligence is built directly into the platform where documentation, billing, and claims performance function as a single unified system.
Because in behavioral health, revenue does not break at billing.
It breaks upstream.